

Combining procalcitonin, c-reactive protein, and white blood cell count in predicting infections in pediatric open cardiac surgery with cardiopulmonary bypass
- PMID: 40373822
- PMCID: PMC12276609
- DOI: 10.1016/j.jped.2025.04.006
Combining procalcitonin, c-reactive protein, and white blood cell count in predicting infections in pediatric open cardiac surgery with cardiopulmonary bypass
Abstract
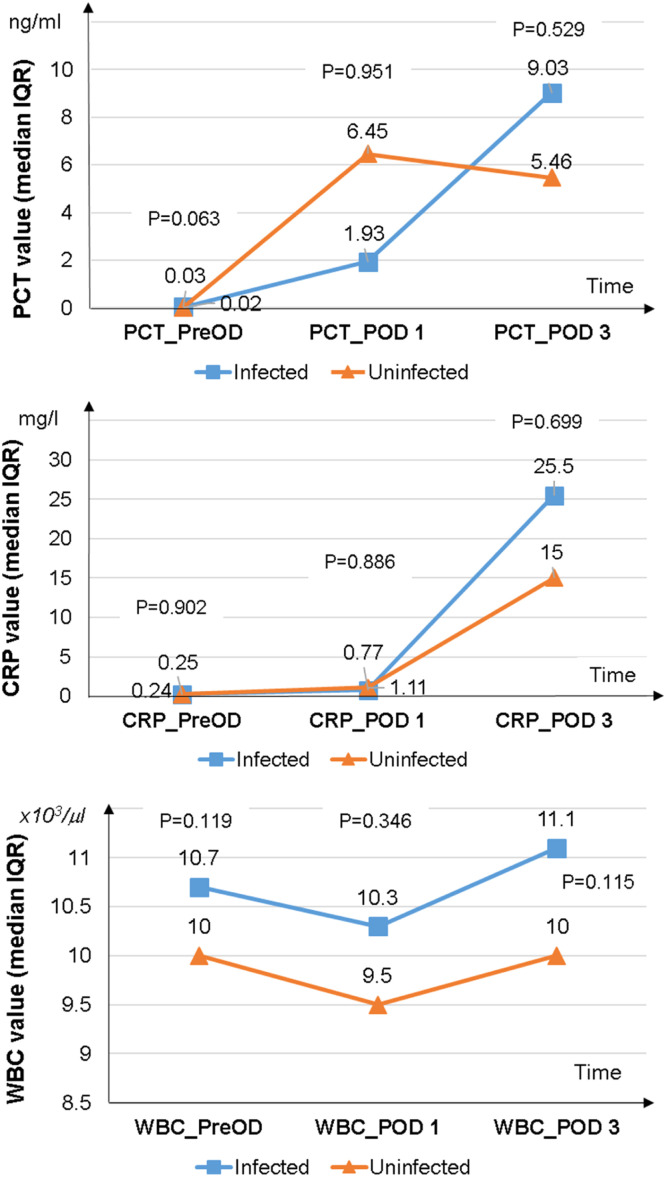
Objective: This study aimed to evaluate the validity of models using Procalcitonin (PCT) alone and PCT combined with other biomarkers to predict early infection after pediatric open-heart surgery with cardiopulmonary bypass (CPB).
Methods: A prospective observational study was conducted on children undergoing open-heart surgery with CPB, without preoperative infection. Procalcitonin, C-reactive protein (CRP), and white blood cell (WBC) count were measured preoperatively and on postoperative days 1 and 3. Postoperative infection was defined according to the Centers for Disease Control and Prevention 2008 criteria.
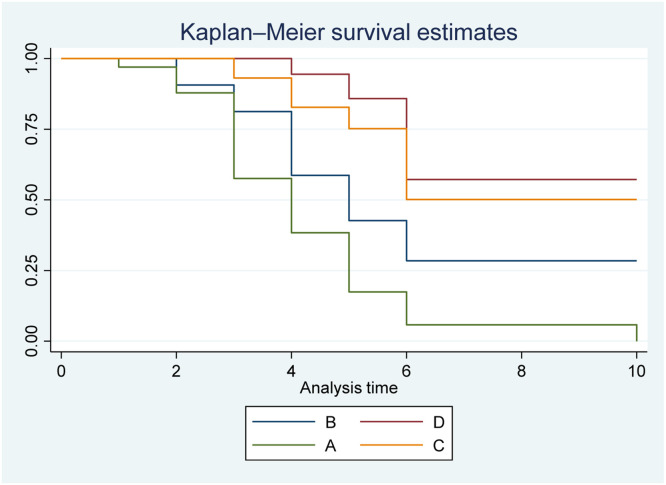
Results: Fifty eligible cases were included, comprising 46 % males with a median age of 7 months (4-17). The AUC (area under the curve) for PCT on postoperative day 3 was 0.67 (0.51-0.82) (p = 0.085). The AUCs for the models combining PCT + CRP and PCT + WBC were 0.71 (0.57-0.86) (p = 0.014) and 0.72 (0.55-0.86) (p = 0.014), respectively. The AUC for the model combining PCT + CRP + WBC was 0.81 (0.69-0.93) (p = 0.002). The combination of PCT > 4.15 ng/ml, CRP > 22.03 mg/l, and WBC > 15.3 × 103/µl predicted infection with a hazard ratio 9.66 times (2.94-31.72) higher than PCT > 4.15 ng/ml alone (p < 0.05).
Conclusions: PCT measurement on the third postoperative day alone cannot predict infection in pediatric open-heart surgery with CPB. The combination of PCT with CRP and WBC may enhance early infection prediction, although further validation in larger, multicenter cohorts is warranted.
Keywords: Cardiopulmonary bypass; Open-heart surgery; Pediatric; Postoperative infections; Procalcitonin.
Copyright © 2025 The Authors. Published by Elsevier Editora Ltda. All rights reserved.
Conflict of interest statement
Conflicts of interest The authors declare no conflicts of interest.
Figures
References
-
- Tönz G.M., Kadner A., Pfammatter J.P., Agyeman P.K. Invasive bacterial and fungal infections after pediatric cardiac surgery: a single-center experience. Pediatr Infect Dis J. 2021;40:310–316. - PubMed
-
- Sochet A.A., Cartron A.M., Nyhan A., Spaeder M.C., Song X., Brown A.T., et al. Surgical site infection after pediatric cardiothoracic surgery. World J Pediatr Congenit Heart Surg. 2017;8:7–12. - PubMed
-
- Whiting D., Yuki K., DiNardo J.A. Cardiopulmonary bypass in the pediatric population. Best Pract Res Clin Anaesthesiol. 2015;29:241–256. - PubMed
-
- Saleem Y., Darbari A., Sharma R., Vashisth A., Gupta A. Recent advancements in pediatric cardiopulmonary bypass technology for better outcomes of pediatric cardiac surgery. Cardiothorac Surg. 2022;30(1) doi: 10.1186/s43057-022-00084-5. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
