

COMPASS: Computational mapping of patient-therapist alliance strategies with language modeling
- PMID: 40374613
- PMCID: PMC12081631
- DOI: 10.1038/s41398-025-03379-3
COMPASS: Computational mapping of patient-therapist alliance strategies with language modeling
Abstract
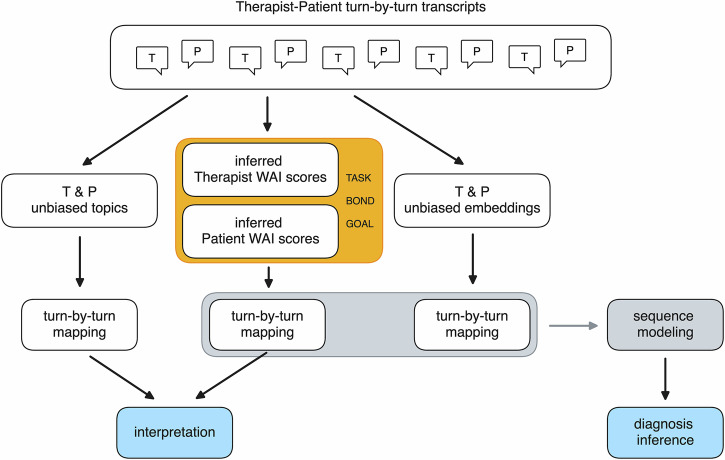
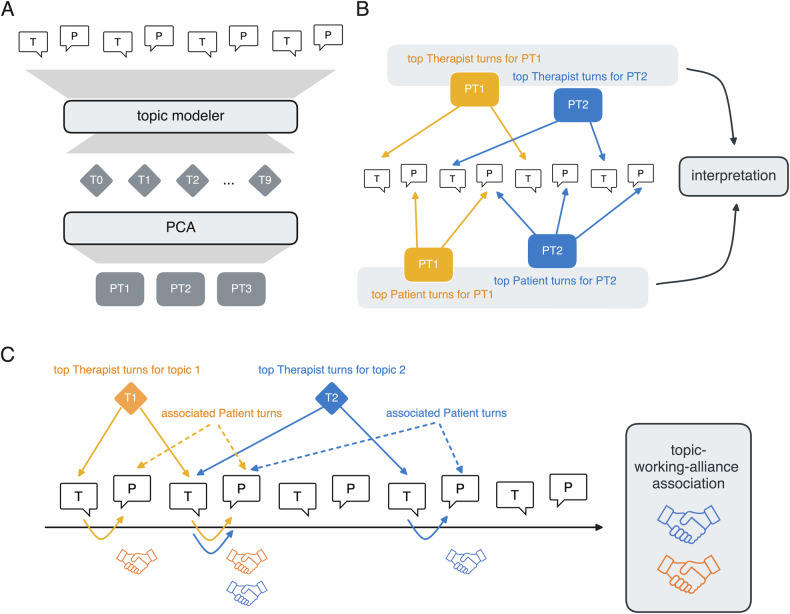
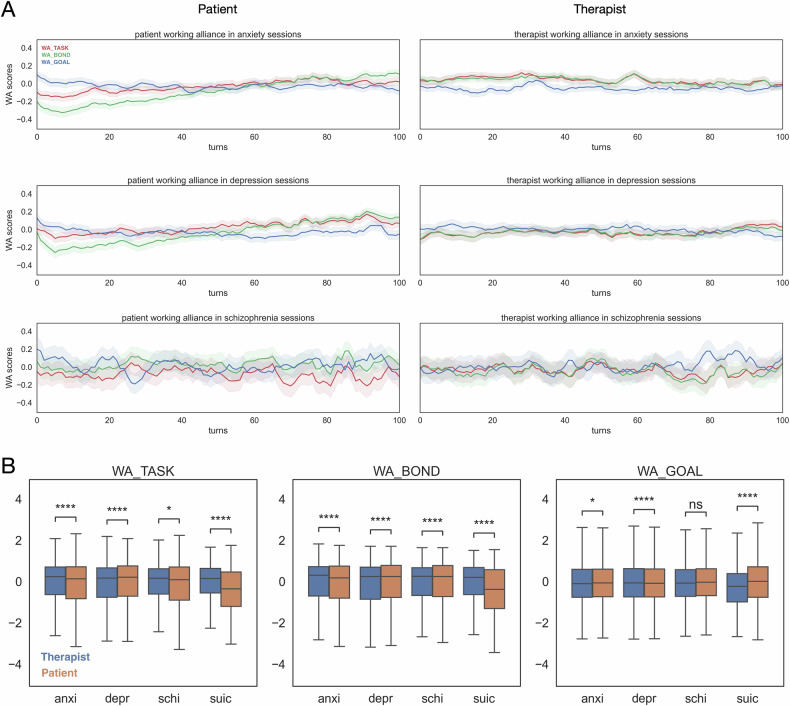
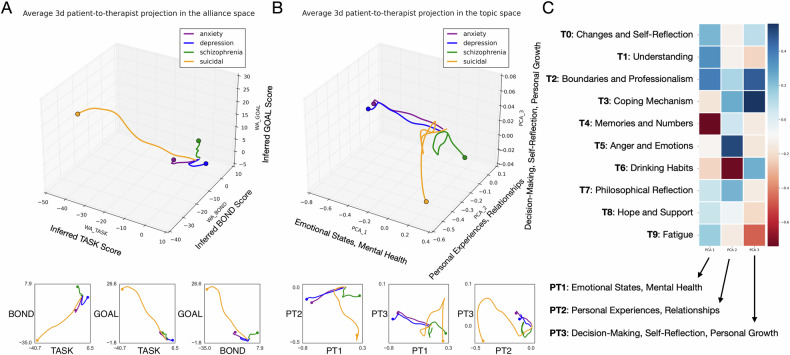
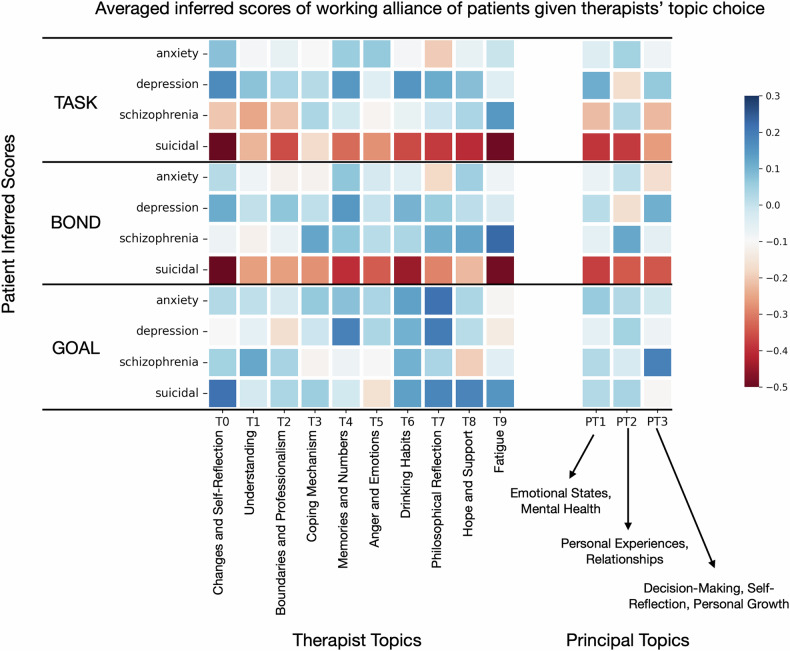
The therapeutic working alliance is a critical predictor of psychotherapy success. Traditionally, working alliance assessment relies on questionnaires completed by both therapists and patients. In this paper, we present COMPASS, a novel framework to directly infer the therapeutic working alliance from the natural language used in psychotherapy sessions. Our approach leverages advanced large language models (LLMs) to analyze session transcripts and map them to distributed representations. These representations capture the semantic similarities between the dialogues and psychometric instruments, such as the Working Alliance Inventory. Analyzing a dataset of over 950 sessions spanning diverse psychiatric conditions -- including anxiety (N = 498), depression (N = 377), schizophrenia (N = 71), and suicidal tendencies (N = 12) -- collected between 1970 and 2012, we demonstrate the effectiveness of our method in providing fine-grained mapping of patient-therapist alignment trajectories, offering interpretable insights for clinical practice, and identifying emerging patterns related to the condition being treated. By employing various deep learning-based topic modeling techniques in combination with prompting generative language models, we analyze the topical characteristics of different psychiatric conditions and how these topics evolve during each turn of the conversation. This integrated framework enhances the understanding of therapeutic interactions, enables timely feedback for therapists on the quality of therapeutic relationships, and provides clear, actionable insights to improve the effectiveness of psychotherapy.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: DB and GC are employees of IBM. All other authors declare no competing interests. Ethics approval and consent to participate statement: This study involved secondary analysis of de-identified, publicly available data. All methods were performed in accordance with relevant guidelines and regulations. As no new data collection from human participants was conducted by the authors, ethics approval and informed consent were not required. Ethical approval and participant consent were obtained by the original data providers, as detailed in the original publications.
Figures
Similar articles
-
Machine learning and natural language processing in psychotherapy research: Alliance as example use case.J Couns Psychol. 2020 Jul;67(4):438-448. doi: 10.1037/cou0000382. J Couns Psychol. 2020. PMID: 32614225 Free PMC article.
-
Measuring Alliance and Symptom Severity in Psychotherapy Transcripts Using Bert Topic Modeling.Adm Policy Ment Health. 2024 Jul;51(4):509-524. doi: 10.1007/s10488-024-01356-4. Epub 2024 Mar 29. Adm Policy Ment Health. 2024. PMID: 38551767 Free PMC article.
-
Patient and therapist perspectives on alliance development: therapists' practice experiences as predictors.Clin Psychol Psychother. 2015 Jul-Aug;22(4):317-27. doi: 10.1002/cpp.1891. Epub 2014 Feb 26. Clin Psychol Psychother. 2015. PMID: 24574034
-
Language style matching in psychotherapy: An implicit aspect of alliance.J Couns Psychol. 2020 Jul;67(4):509-522. doi: 10.1037/cou0000433. J Couns Psychol. 2020. PMID: 32614231 Review.
-
Alliance rupture and repair in adolescent psychotherapy: What clinicians can learn from research.Psychotherapy (Chic). 2024 Dec;61(4):304-313. doi: 10.1037/pst0000535. Epub 2024 Jul 18. Psychotherapy (Chic). 2024. PMID: 39023966 Review.
References
-
- Bordin ES. The generalizability of the psychoanalytic concept of the working alliance. Psychother Theory Res Pract. 1979;16:252.
-
- Horvath AO, Greenberg LS. The working alliance: theory, research, and practice. John Wiley & Sons; New York, NY; 1994. 173.
-
- Norcross JC. The therapeutic relationship. In BL, Duncan SD, Miller BE, Hubble WMA, editors. The heart and soul of change: Delivering what works in therapy. American Psychological Association. 2010. pp. 113–141.
-
- Eliacin J, Coffing JM, Matthias MS, Burgess DJ, Bair MJ, Rollins AL. The relationship between race, patient activation, and working alliance: implications for patient engagement in mental health care. Adm Policy Ment Health Ment Health Serv Res. 2018;45:186–92. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
