

Pneumococcal vaccine hyporesponsiveness in people living with HIV: A narrative review of immunological mechanisms and insights from minimally invasive lymph node sampling
- PMID: 40374620
- PMCID: PMC12087491
- DOI: 10.1080/21645515.2025.2503602
Pneumococcal vaccine hyporesponsiveness in people living with HIV: A narrative review of immunological mechanisms and insights from minimally invasive lymph node sampling
Abstract
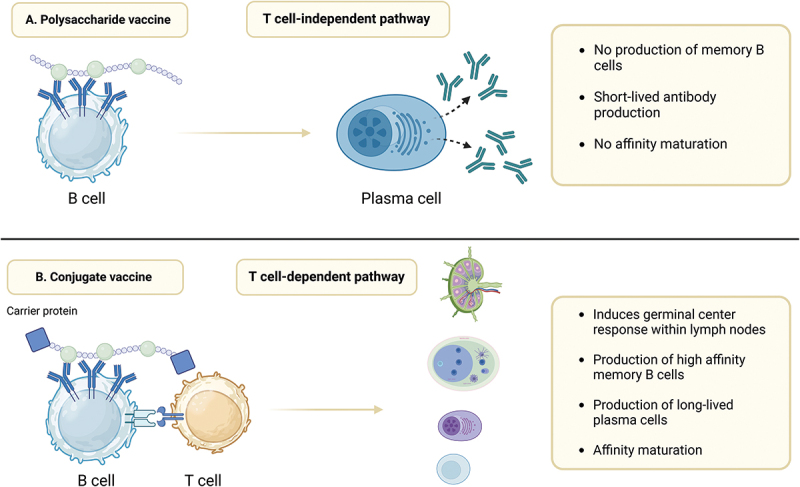
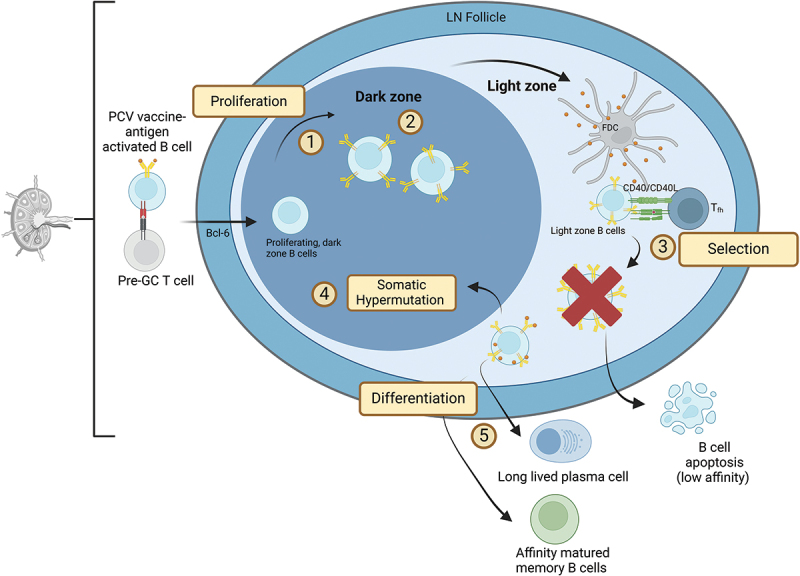
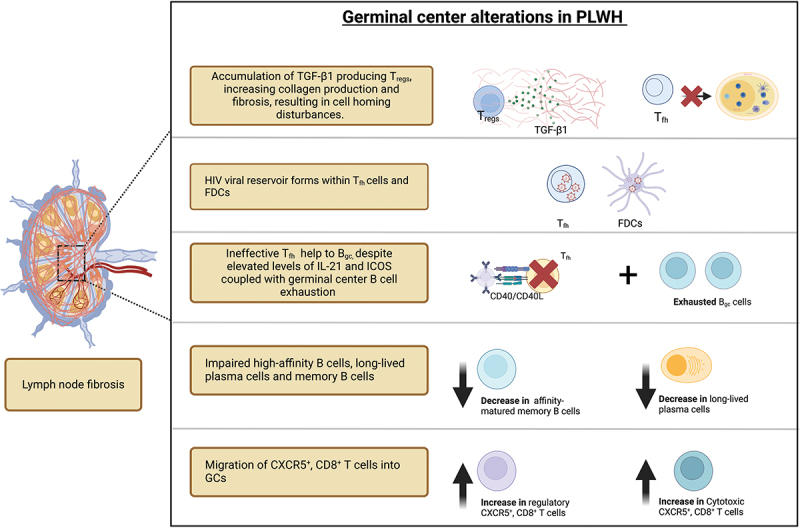
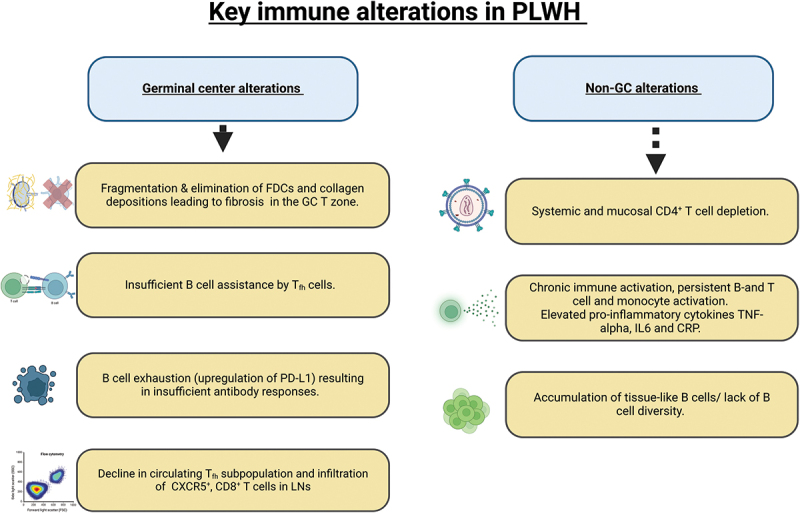
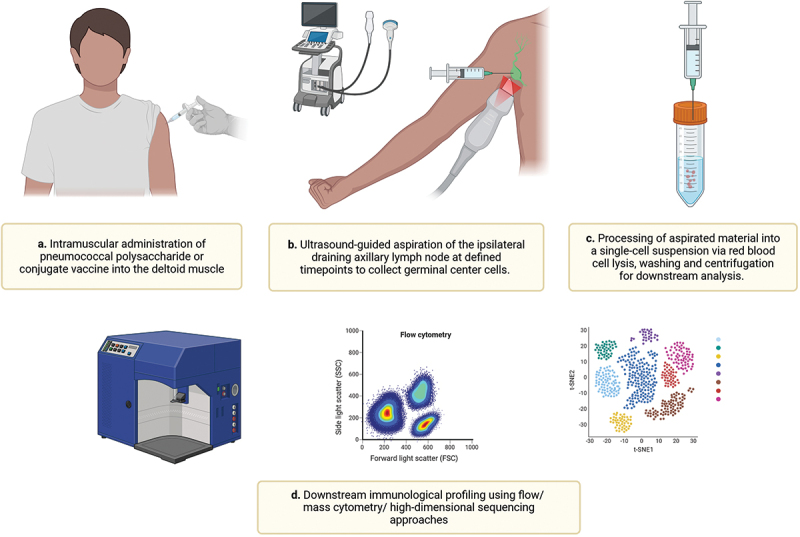
Despite highly effective antiretroviral therapy, people living with HIV (PLWH) remain at elevated risk for invasive pneumococcal disease. Clinical studies show that, even with high CD4+ counts, PLWH exhibit diminished serological responses and rapid antibody decline following pneumococcal vaccination, plausibly due to underlying immune dysfunction. Germinal centers (GCs), located within lymph nodes, are essential for generating high-affinity antibodies, but are structurally and functionally disrupted in PLWH. These local impairments, combined with systemic immune dysregulation, contribute to vaccine hyporesponsiveness in PLWH. This narrative review links immunological findings from experimental and in vivo studies to clinical pneumococcal vaccine trials, to investigate mechanisms that may be leveraged to strengthen vaccine-induced immunity in PLWH. We also highlight the application of fine needle aspiration (FNA) of the lymph node as a way to study pneumococcal vaccine hyporesponsiveness in the GC and provide potential direction to improve responses for next-generation pneumococcal conjugate vaccines in PLWH.
Keywords: Pneumococcal vaccination; germinal centers; lymph node fine-needle aspiration; people living with HIV; pneumococcal conjugate vaccine; pneumococcal polysaccharide vaccine.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
Similar articles
-
Immunogenicity of the 13-valent pneumococcal conjugate vaccine followed by the 23-valent pneumococcal polysaccharide vaccine in people living with HIV on combination antiretroviral therapy.Int J Antimicrob Agents. 2022 Aug;60(2):106629. doi: 10.1016/j.ijantimicag.2022.106629. Epub 2022 Jun 24. Int J Antimicrob Agents. 2022. PMID: 35760223
-
Single-Dose 13-Valent Conjugate Pneumococcal Vaccine in People Living With HIV - Immunological Response and Protection.Front Immunol. 2021 Dec 20;12:791147. doi: 10.3389/fimmu.2021.791147. eCollection 2021. Front Immunol. 2021. PMID: 34987514 Free PMC article.
-
Serologic response to primary vaccination with 7-valent pneumococcal conjugate vaccine is better than with 23-valent pneumococcal polysaccharide vaccine in HIV-infected patients in the era of combination antiretroviral therapy.Hum Vaccin Immunother. 2013 Feb;9(2):398-404. doi: 10.4161/hv.22836. Epub 2013 Jan 4. Hum Vaccin Immunother. 2013. PMID: 23291936 Free PMC article.
-
Immunogenicity following revaccination or sequential vaccination with 23-valent pneumococcal polysaccharide vaccine (PPSV23) in older adults and those at increased risk of pneumococcal disease: a review of the literature.Expert Rev Vaccines. 2021 Mar;20(3):257-267. doi: 10.1080/14760584.2021.1889374. Epub 2021 Mar 2. Expert Rev Vaccines. 2021. PMID: 33567914 Review.
-
Pneumococcal Vaccination Strategies Among HIV-infected Adult Patients: A Review of the Literature.In Vivo. 2019 Sep-Oct;33(5):1425-1430. doi: 10.21873/invivo.11620. In Vivo. 2019. PMID: 31471388 Free PMC article. Review.
References
-
- Barre-Sinoussi F, Chermann JC, Rey F, Nugeyre MT, Chamaret S, Gruest J, Dauguet C, Axler-Blin C, Vézinet-Brun F, Rouzioux C, et al. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). Science. 1983;220(4599):868–17. doi: 10.1126/science.6189183. - DOI - PubMed
-
- Wong CS, Buckner CM, Lage SL, Pei L, Assis FL, Dahlstrom EW, Anzick SL, Virtaneva K, Rupert A, Davis JL, et al. Rapid emergence of T follicular helper and germinal center B cells following antiretroviral therapy in advanced HIV disease. Front Immunol. 2021;12:752782. doi: 10.3389/fimmu.2021.752782. - DOI - PMC - PubMed
-
- Organization WH. Epidemiological fact sheet: HIV statistics, globally and by WHO region, 2023. World Health Organ. 2023.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous