

Cost-effectiveness of low-dose CT screening for non-smokers with a first-degree relative history of lung cancer
- PMID: 40375086
- PMCID: PMC12079829
- DOI: 10.1186/s12889-025-22977-w
Cost-effectiveness of low-dose CT screening for non-smokers with a first-degree relative history of lung cancer
Abstract
Background: Lung cancer is the leading cause of cancer-related deaths worldwide, with non-smokers in China accounting for over 40% of cases. Despite the proven efficacy of low-dose computed tomography (LDCT) in early detection and reduction of lung cancer mortality, the current paradigm of lung cancer screening, heavily focused on smoking status and age, may inadequately address the unique risk factors associated with non-smokers, particularly those with a family history of the disease. This study evaluates the cost-effectiveness of LDCT screening for non-smokers with a first-degree relative (FDR) history of lung cancer, a group at particularly high-risk.
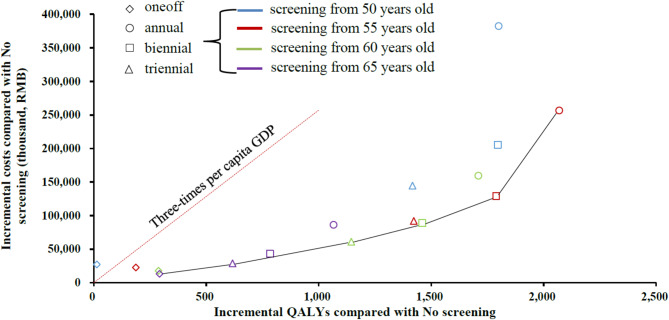
Methods: We developed a state-transition Markov model to evaluate the incremental cost-effectiveness ratios (ICERs) of 16 screening strategies for a hypothetical cohort of 100,000 non-smoking individuals aged 50 with a FDR history of lung cancer, considering various starting ages (50, 55, 60, 65 years) and intervals (one-off, annual, biennial, triennial). The willingness-to-pay (WTP) threshold was set at three times China's 2022 per-capita GDP. Sensitivity analyses, scenario analyses and subgroup analysis by sex, were conducted.
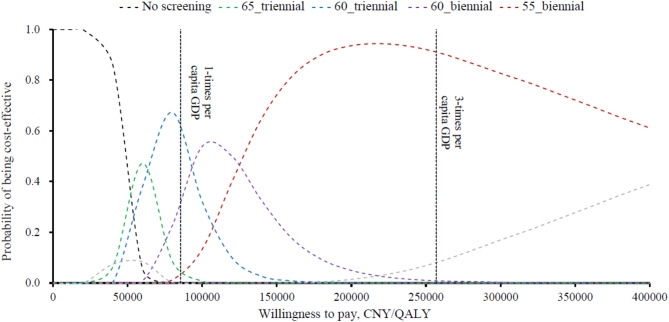
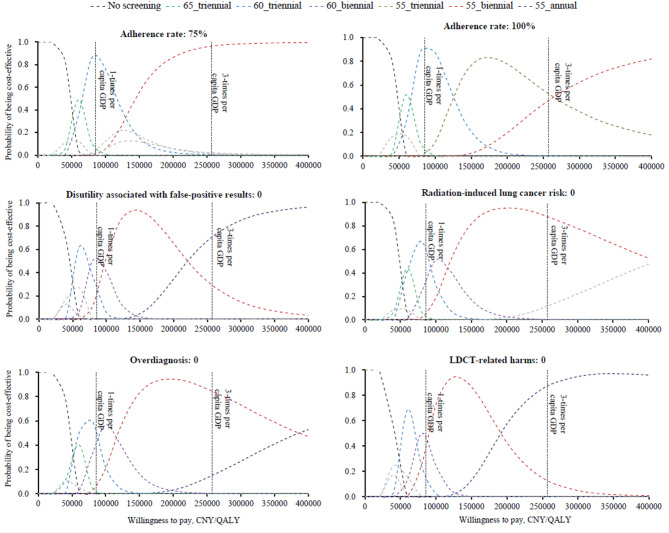
Results: Compared to no screening, all strategies except one-off screening at age 50, were cost-effective for both sexes. Biennial LDCT starting at age 55 was found to be most effective, with an ICER of CNY 68,932/QALY for males, and CNY 80,056/QALY for females. This cost-effectiveness probability for this strategy was approximately 90% for both sexes. Sensitivity analyses indicated that annual screening at age 55 was optimal without discounting. For males, biennial at age 60 was optimal if the FDR-related odds ratio for lung cancer incidence was below 1.492. Triennial screening at age 55 was optimal for females at full adherence. Ignoring disutility from false-positive results, annual at age 55 was optimal for both sexes.
Conclusions: LDCT screening for non-smokers with a FDR history of lung cancer is cost-effective, especially biennial screening at 55. These findings support the development of more inclusive screening guidelines, which could enhance early detection and reduce mortality rates.
Keywords: Cost-effectiveness; LDCT screening; Lung Cancer; Modelling study; Non-smokers.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–63. - PubMed
-
- Global Cancer Observatory. International Agency for Research on Cancer. https://gco.iarc.fr/en. Accessed March 10, 2024.
-
- de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer mortality with volume CT screening in a randomized trial. N Engl J Med. 2020;382(6):503–13. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
