

Readiness of health facilities to deliver family planning services and associated factors in urban east-central Uganda
- PMID: 40375305
- PMCID: PMC12083106
- DOI: 10.1186/s12978-025-02026-w
Readiness of health facilities to deliver family planning services and associated factors in urban east-central Uganda
Abstract
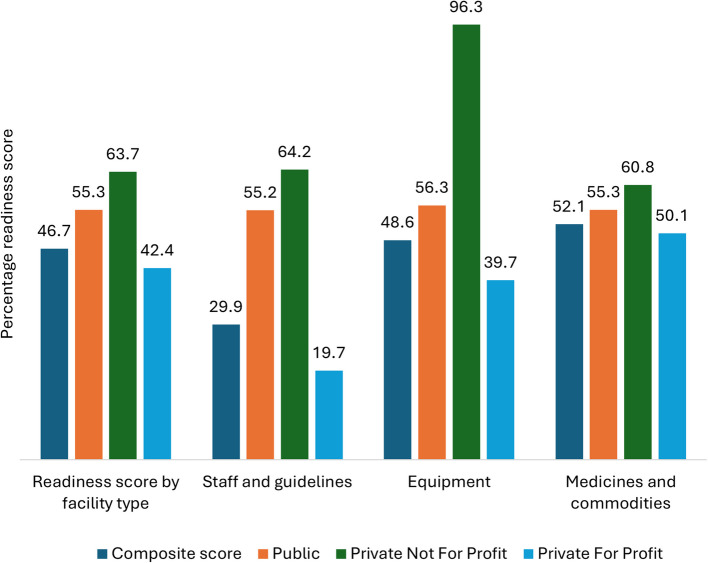
Background: Health facility readiness is essential for realizing voluntary, rights-based family planning. However, many countries, including rapidly urbanizing Uganda, face challenges in ensuring their health facilities are sufficiently equipped to meet the growing demand for these services. This study assessed readiness and associated factors across public, private-not-for-profit (PNFP), and private-for-profit (PFP) health facilities in urban east-central Uganda to guide strategies for improving service delivery.
Methods: The study used secondary data from a cross-sectional study done in Jinja City and Iganga Municipality, including a health facility assessment and health worker survey. Readiness was measured using the Service Availability and Readiness Assessment methodology, and health worker knowledge and biases were assessed through the Situation Analysis approach. Sample weights adjusted for facility and health worker representation, and linear regression examined associations between readiness scores and various factors.
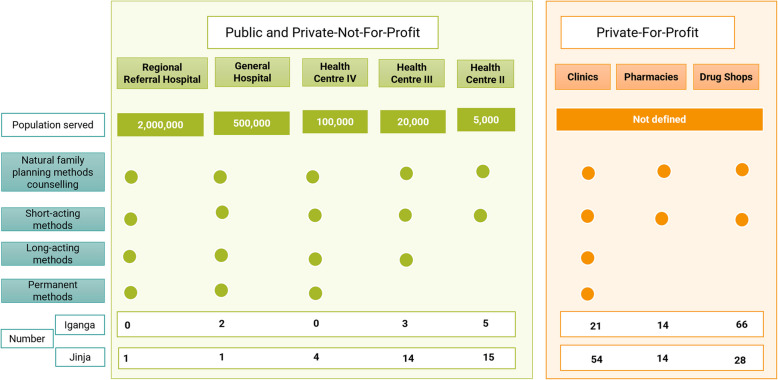
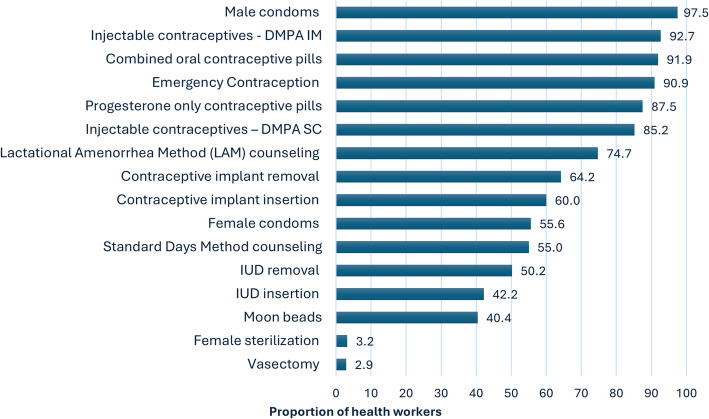
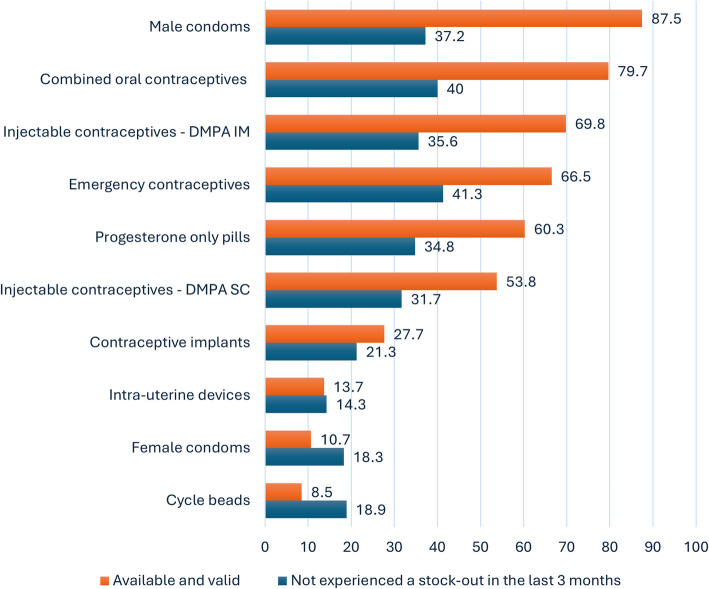
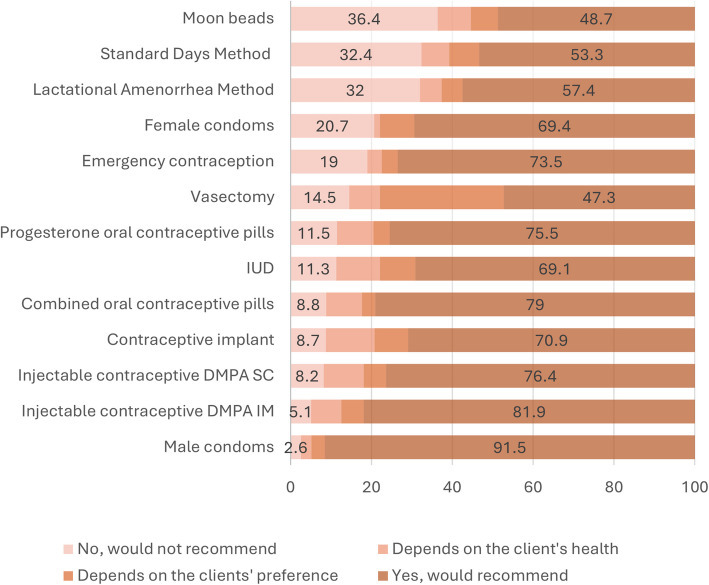
Results: Among 152 health facilities, 94.2% offered family planning services, with an average readiness score of 46.7% (standard deviation ± 17.0). Short-acting methods had high availability (99.0%), while long-acting reversible contraceptives (34.2%) and permanent options (8.9%) were less available, compounded by prevalent stock-outs. Additionally, staff refresher training was inadequate, particularly in PFP facilities (50.4%), and health worker knowledge, confidence and willingness to provide some methods, particularly long-acting options and natural family planning counselling, were low. Notably, out of 261 health workers, 97.7% imposed at least one restriction to service access based on either age, parity, marital status, or spousal consent, more pronounced in PNFP facilities. Readiness was significantly associated with facility level (health centre level II facilities: β = -9.42, p = 0.036; drug shops: β = -11.00, p = 0.022), external supervision (β = 9.04, p = 0.009), holding administrative meetings (β = 9.72, p = 0.017), and imposing marital status (β = -9.42, p = 0.017) and spousal consent access barriers (β = 6.24, p = 0.023).
Conclusions: This study found sub-optimal facility readiness, highlighting the need to strengthen governance of services across both public and private sectors, implement comprehensive training for health workers in both sectors, and align policies to ensure equitable access to a full range of services for all clients.
Keywords: Access barriers; Family Planning; Health facility readiness; Uganda; Urban.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval for the study was granted by the Makerere University School of Public Health Research and Ethics Committee (REC) (Reference Number: SPH-2023–384) and the Uganda National Council for Science and Technology (UNCST) (Reference Number: HS3222ES). The Urban Thrive Project, whose data was utilized for this study, also received approval from the Makerere University School of Public Health REC (Reference Number: SPH-2021–146) and UNCST (Reference Number: HS1826ES). In addition, administrative clearance was obtained from the leadership of Jinja City and Iganga Municipality. All health facilities provided authorization to be included in the study while the health workers interviewed provided written informed consent prior to their participation. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Facilitators, best practices and barriers to integrating family planning data in Uganda's health management information system.BMC Health Serv Res. 2019 May 22;19(1):327. doi: 10.1186/s12913-019-4151-9. BMC Health Serv Res. 2019. PMID: 31118006 Free PMC article.
-
Assessment of Family Planning Service Availability and Readiness in 10 African Countries.Glob Health Sci Pract. 2018 Oct 4;6(3):473-483. doi: 10.9745/GHSP-D-18-00041. Print 2018 Oct 3. Glob Health Sci Pract. 2018. PMID: 30213877 Free PMC article.
-
Assessment of the readiness of health facilities in urban areas to deliver geriatric-friendly care services: a cross-sectional study in Kampala City, Uganda.BMC Geriatr. 2024 Sep 25;24(1):786. doi: 10.1186/s12877-024-05353-y. BMC Geriatr. 2024. PMID: 39322965 Free PMC article.
-
Services availability and readiness assessment of adolescent sexual and reproductive health in primary healthcare facilities: evidence from selected districts in Ghana.Reprod Health. 2025 Feb 1;22(1):14. doi: 10.1186/s12978-025-01955-w. Reprod Health. 2025. PMID: 39893462 Free PMC article.
-
Measuring availability of and facility readiness to deliver comprehensive abortion care: experiences and lessons learnt from integrating abortion into WHO's health facility assessments.BMJ Glob Health. 2024 Aug 9;8(Suppl 4):e015097. doi: 10.1136/bmjgh-2024-015097. BMJ Glob Health. 2024. PMID: 39122445 Free PMC article. Review.
References
-
- Prata N. The need for family planning. Popul Environ. 2007;28(4):212–22.
-
- United Nations Population Fund. Family planning is a human right 2018. Available from: https://www.unfpa.org/press/family-planning-human-right.
-
- Jain AK, Hardee K. Revising the FP quality of care framework in the context of rights-based family planning. Stud Fam Plann. 2018;49(2):171–9. - PubMed
-
- Bruce J. Fundamental elements of the quality of care: a simple framework. Stud Fam Plann. 1990;21(2):61–91. - PubMed
-
- RamaRao S, Mohanam R. The quality of family planning programs: concepts, measurements, interventions, and effects. Stud Fam Plann. 2003;34(4):227–48. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
