

Enhanced Closed Incisional Negative Pressure Therapy for Treating Infectious Scars
- PMID: 40375957
- PMCID: PMC12080673
- DOI: 10.1097/GOX.0000000000006776
Enhanced Closed Incisional Negative Pressure Therapy for Treating Infectious Scars
Abstract
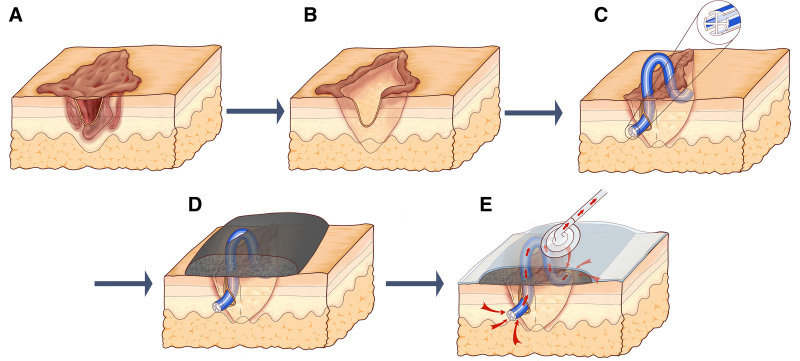
Background: Chronic infectious pathological scars, characterized by mutual reinforcement between infection and pathological scarring, pose challenges in reconstructive surgery. We introduce an enhanced closed incisional negative pressure therapy following a 1-stage surgery to simultaneously eradicate infection and alleviate wound tension.
Methods: A total of 25 patients who underwent chronic infectious pathological scar treatment by using this enhanced closed incisional negative pressure therapy were retrospectively reviewed. The outcomes were evaluated by postoperative recurrence frequency of infection and scarring during a 1-year follow-up, as well as the Patient and Observer Scar Assessment Scale and quality-of-life scores.
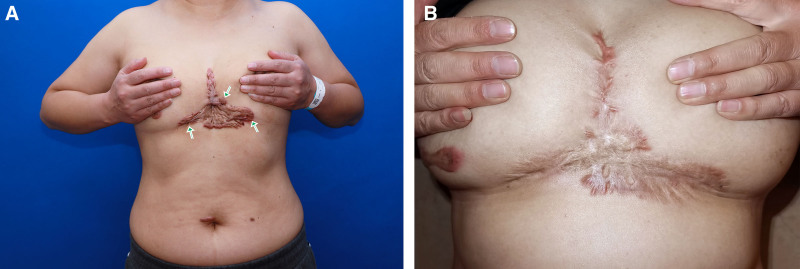
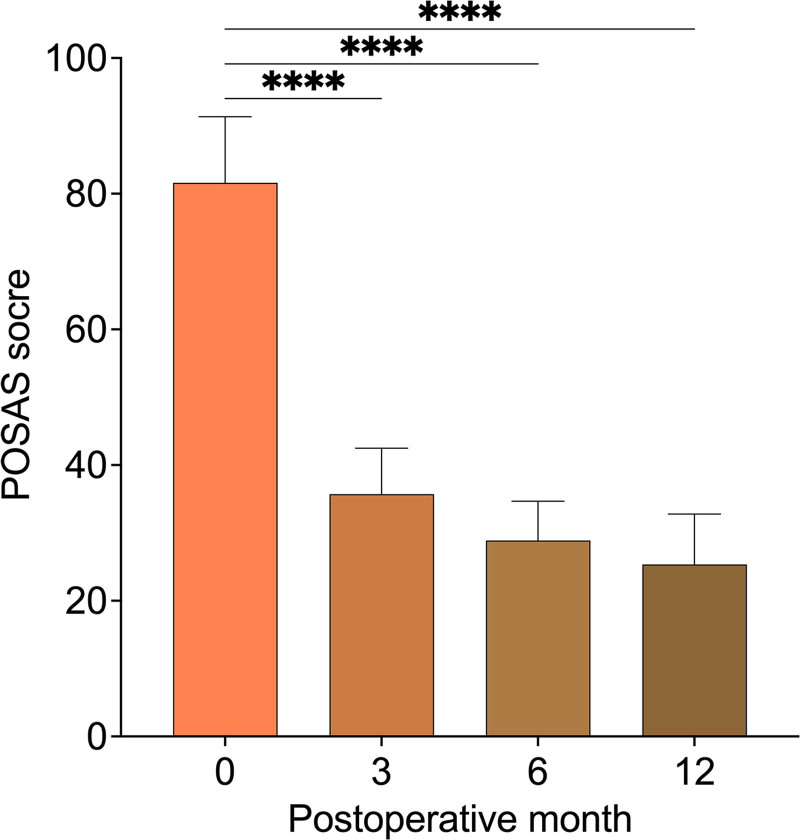
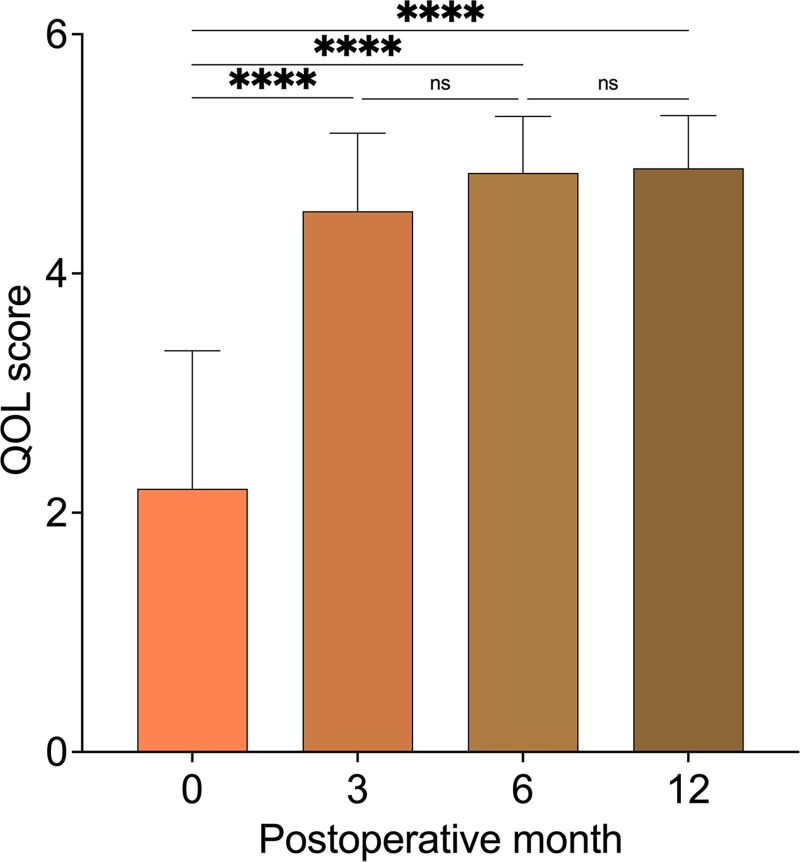
Results: After treatment, no serious complications, such as incision dehiscence, occurred. The average wound healing time was 12.68 days. Only 1 patient experienced surgical site scarring. Besides, average infection frequency decreased significantly from 6.40 to 0.00 times per year (P < 0.0001). The Patient and Observer Scar Assessment Scale score decreased from 81.60 to 25.36 (P < 0.0001), whereas the quality-of-life score increased from 2.20 to 4.88 (P < 0.0001).
Conclusions: The enhanced closed incisional negative pressure therapy effectively facilitated infectious wound healing in a 1-stage operation and simultaneously prevented infection and scarring recurrence in long-term follow-up, resulting in satisfactory postoperative outcomes.
Copyright © 2025 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
The authors have no financial interest to declare in relation to the content of this article. This study was supported by grants from the National Natural Science Foundation of China (82372535), the Shanghai Clinical Research Center of Plastic and Reconstructive Surgery supported by the Science and Technology Commission of Shanghai Municipality (22MC1940300), and the Shanghai Municipal Key Clinical Specialty (shslczdzk00901).
Figures
Similar articles
-
Negative-pressure wound therapy compared with standard dressings following surgical treatment of major trauma to the lower limb: the WHiST RCT.Health Technol Assess. 2020 Aug;24(38):1-86. doi: 10.3310/hta24380. Health Technol Assess. 2020. PMID: 32821038 Free PMC article. Clinical Trial.
-
The impact of closed incisional negative pressure therapy on anterior lateral thigh flap donor site healing and scarring: A retrospective case-control study.J Plast Reconstr Aesthet Surg. 2022 Jan;75(1):152-159. doi: 10.1016/j.bjps.2021.05.049. Epub 2021 Jun 13. J Plast Reconstr Aesthet Surg. 2022. PMID: 34274247
-
Use of prophylactic closed incision negative pressure therapy is associated with reduced surgical site infections in gynecologic oncology patients undergoing laparotomy.Am J Obstet Gynecol. 2020 Nov;223(5):731.e1-731.e9. doi: 10.1016/j.ajog.2020.05.011. Epub 2020 May 15. Am J Obstet Gynecol. 2020. PMID: 32417358
-
A systematic review evaluating the influence of incisional Negative Pressure Wound Therapy on scarring.Wound Repair Regen. 2021 Jan;29(1):8-19. doi: 10.1111/wrr.12858. Epub 2020 Aug 21. Wound Repair Regen. 2021. PMID: 32789902 Free PMC article.
-
Incisional negative pressure wound therapy for high-risk wounds.J Wound Care. 2015 Apr;24(4 Suppl):21-8. doi: 10.12968/jowc.2015.24.Sup4b.21. J Wound Care. 2015. PMID: 25853645 Review.
References
-
- Elsaie ML. Update on management of keloid and hypertrophic scars: a systemic review. J Cosmet Dermatol. 2021;20:2729–2738. - PubMed
-
- Huang C, Wu Z, Du Y, Ogawa R. The epidemiology of keloids. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, eds. Textbook on Scar Management: State of the Art Management and Emerging Technologies. Springer; 2020;Chapter 4. - PubMed
LinkOut - more resources
Full Text Sources