

A 51-Year-Old Woman With Subarachnoid Hemorrhage and Secondary Central Nervous System Vasculitis With Progression to Diffuse, Serpiginous Dolichoectasia
- PMID: 40376103
- PMCID: PMC12075185
- DOI: 10.1177/19418744251336501
A 51-Year-Old Woman With Subarachnoid Hemorrhage and Secondary Central Nervous System Vasculitis With Progression to Diffuse, Serpiginous Dolichoectasia
Abstract
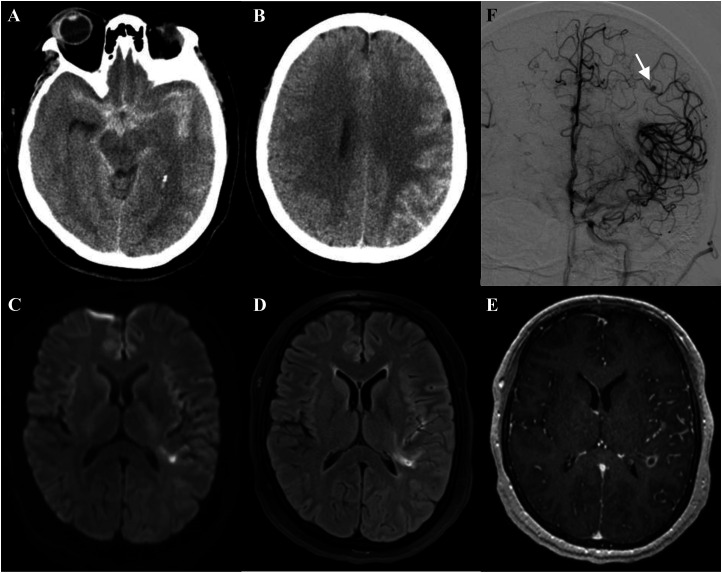
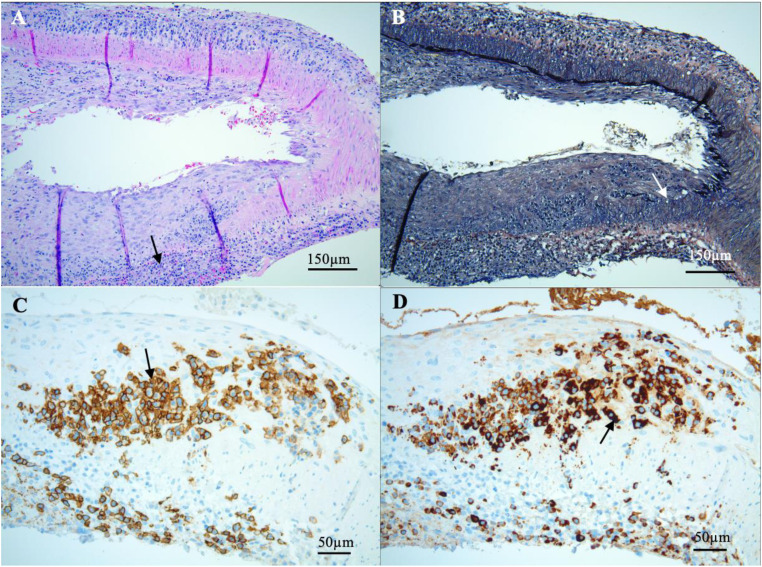
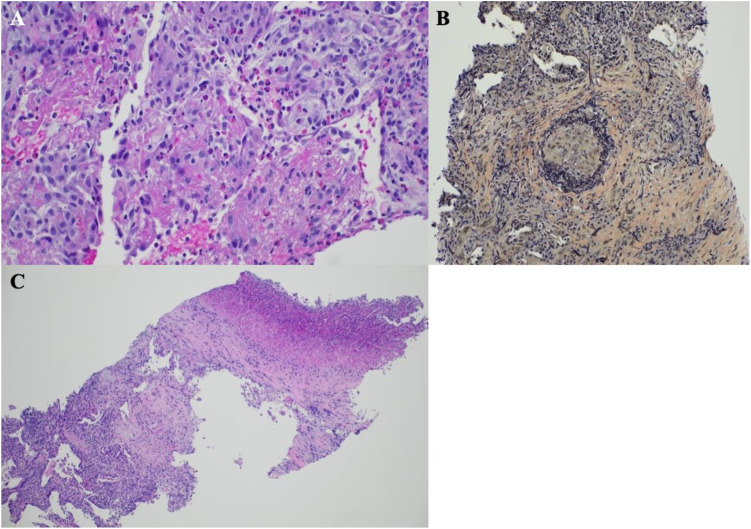
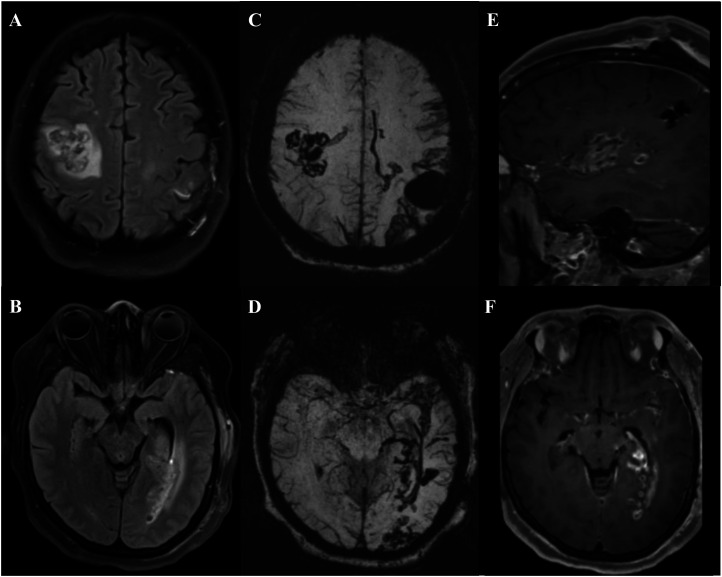
A 51-year-old woman presented with acute onset of a severe headache, and was found to have diffuse subarachnoid hemorrhage with prominent cisternal and left cortical convexity blood on head computed tomography. The first 2 conventional angiograms were negative for aneurysm, but a third angiogram revealed a mycotic aneurysm of a distal left middle cerebral artery branch. Brain biopsy, associated with clipping of the aneurysm, demonstrated pathology consistent with vasculitis. Over the course of a month, she developed diffuse, serpiginous dolichoectasia of the cerebral arteries. Further investigation into the cause of vasculitis supported a diagnosis of either eosinophilic granulomatosis with polyangiitis (EGPA) or IgG4-Related Disease (IgG4-RD). The following clinical pathologic conference discusses the diagnostic challenges in discriminating between these 2 diseases, particularly in the setting of secondary angiitis of the central nervous system.
Keywords: CNS vasculitis; IgG4-related; dilating arteriopathy; disease; dolichoectasia; eosinophilic granulomatosis with polyangiitis; mycotic aneurysm.
© The Author(s) 2025.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Catastrophic subarachnoid hemorrhage in eosinophilic granulomatosis with polyangiitis without asthma.Int J Rheum Dis. 2017 Dec;20(12):2127-2131. doi: 10.1111/1756-185X.12594. Epub 2015 May 11. Int J Rheum Dis. 2017. PMID: 25959920
-
Eosinophilic granulomatosis with polyangiitis complicated by subarachnoid hemorrhage and coronary vasculitis: a case report and review of the literature.Rheumatol Int. 2018 Apr;38(4):689-696. doi: 10.1007/s00296-017-3875-2. Epub 2017 Nov 10. Rheumatol Int. 2018. PMID: 29127573 Review.
-
Subarachnoid Hemorrhaging with Multiple Cerebral Artery Stenoses after Initiating Remission Induction Therapy for Eosinophilic Granulomatosis with Polyangiitis.Intern Med. 2024 Dec 15;63(24):3389-3394. doi: 10.2169/internalmedicine.3583-24. Epub 2024 May 9. Intern Med. 2024. PMID: 38719596 Free PMC article.
-
IgG4-Related Disease: A New Etiology Underlying Diffuse Intracranial Dilating Vasculopathy.World Neurosurg. 2017 Nov;107:1048.e15-1048.e20. doi: 10.1016/j.wneu.2017.08.012. Epub 2017 Aug 10. World Neurosurg. 2017. PMID: 28803167
-
Coexistence of IgG4-related disease and ANCA-associated vasculitis: case report and review of the literature.Rheumatol Int. 2024 Mar;44(3):557-572. doi: 10.1007/s00296-023-05419-x. Epub 2023 Aug 27. Rheumatol Int. 2024. PMID: 37634133 Review.
References
-
- Brust JCM, Dickinson PCT, Hughes JEO, Holtzman RNN. The diagnosis and treatment of cerebral mycotic aneurysms. Ann Neurol. 1990;27:238-246. - PubMed
-
- Refai D, Botros JA, Strom RG, Derdeyn CP, Sharma A, Zipfel GJ. Spontaneous isolated convexity subarachnoid hemorrhage: presentation, radiological findings, differential diagnosis, and clinical course: clinical article. J Neurosurg. 2008;109:1034-1041. - PubMed
-
- Ziment I. Nervous system complications in bacterial endocarditis. Am J Med. 1969;47:593-607. - PubMed
-
- Salvarani C, Brown RD, Jr, Calamia KT, et al. Primary central nervous system vasculitis: analysis of 101 patients. Ann Neurol. 2007;62:442-451. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous