

Efficacies of radiotherapy in rectal cancer patients treated with total mesorectal excision or other types of surgery: an updated meta-analysis
- PMID: 40376112
- PMCID: PMC12078337
- DOI: 10.3389/or.2025.1567818
Efficacies of radiotherapy in rectal cancer patients treated with total mesorectal excision or other types of surgery: an updated meta-analysis
Abstract
Background: An updated meta-analysis was conducted to evaluate the efficacy of radiotherapy in rectal cancer patients treated with total mesorectal excision (TME) or other types of surgery (non-TME-only).
Methods: The PubMed, Cochrane Library, and CNKI databases were searched. Data on overall survival (OS) were extracted.
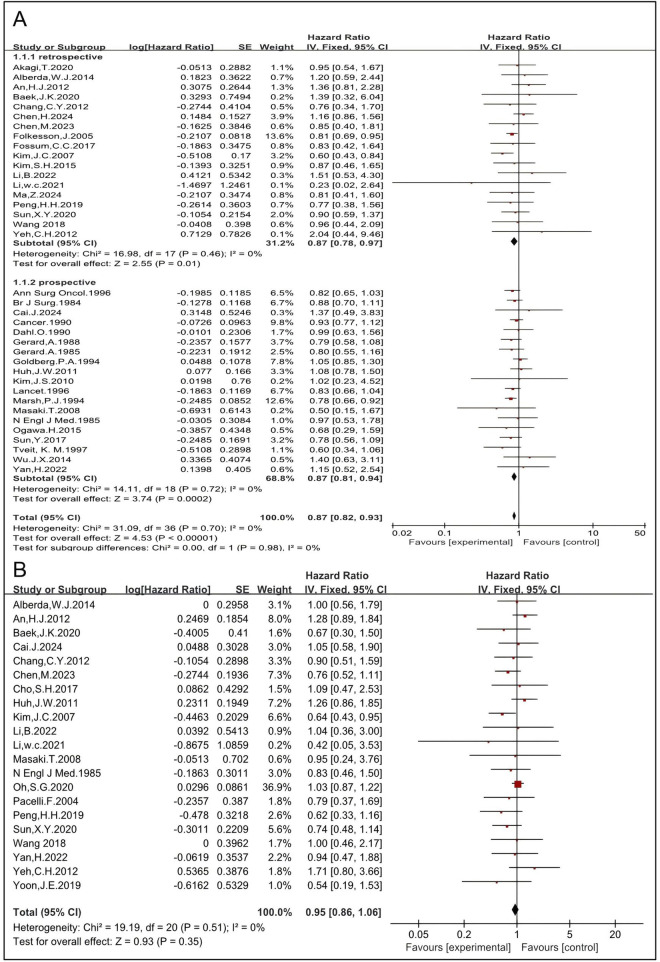
Results: Hazard ratios (HRs) for OS associated with preoperative radiotherapy, preoperative long-course concurrent chemoradiotherapy (LCCRT), preoperative radiotherapy alone, and postoperative radiotherapy in patients treated with TME were 1.02 [95% CI: 0.92-1.14, P = 0.65], 1.04 [95% CI: 0.93-1.16, P = 0.47], 0.87 [95% CI: 0.61-1.25, P = 0.46], and 1.18 [95% CI: 0.91-1.52, P = 0.20], respectively. HRs for OS associated with preoperative radiotherapy, preoperative LCCRT, preoperative radiotherapy alone, preoperative long-course RT (LCRT), and preoperative short-course radiotherapy (SCRT) in patients treated with non-TME-only surgery were 0.85 [95% CI: 0.79-0.90, P < 0.00001], 0.77 [95% CI: 0.63-0.94, P = 0.009], 0.86 [95% CI: 0.80-0.92, P < 0.0001], 0.83 [95% CI: 0.73-0.95, P = 0.005], and 0.84 [95% CI: 0.77-0.91, P= <0.0001], respectively. The HR for postoperative radiotherapy in patients treated with non-TME-only surgery was 1.08 [95% CI: 0.84-1.39, P = 0.57].
Conclusion: Preoperative radiotherapy, regardless of the regimen, improves the OS in patients treated with non-TME-only surgery, but not in those treated with TME. Postoperative radiotherapy does not improve OS.
Advances in knowledge: This meta-analysis will serve as a reference for decision-making in multidisciplinary approaches for rectal cancer patients.
Keywords: TME; concurrent chemoradiotherapy; radiotherapy; rectal cancer; surgery.
Copyright © 2025 Wang, Zhao, Liang, Liu, Bai, Ge, Yao, Zhi and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures









References
-
- Stockholm Rectal Cancer Study Group. Preoperative short-term radiation therapy in operable rectal carcinoma: a prospective randomized trial. Cancer. (1990) 66(1):49–55. 10.1002/1097-0142(19900701)66.1<4910.1002/1097-0142(19900701)66:1<49::aid-cncr2820660111>3.0.co;2-1aid-cncr2820660111>3.0.co - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources