

Natural Orifice Specimen Extraction for Right-Sided Colon Cancer: A Systematic Review and Meta-Analysis of Propensity Score-Matched Studies
- PMID: 40376134
- PMCID: PMC12081068
- DOI: 10.7759/cureus.84191
Natural Orifice Specimen Extraction for Right-Sided Colon Cancer: A Systematic Review and Meta-Analysis of Propensity Score-Matched Studies
Abstract
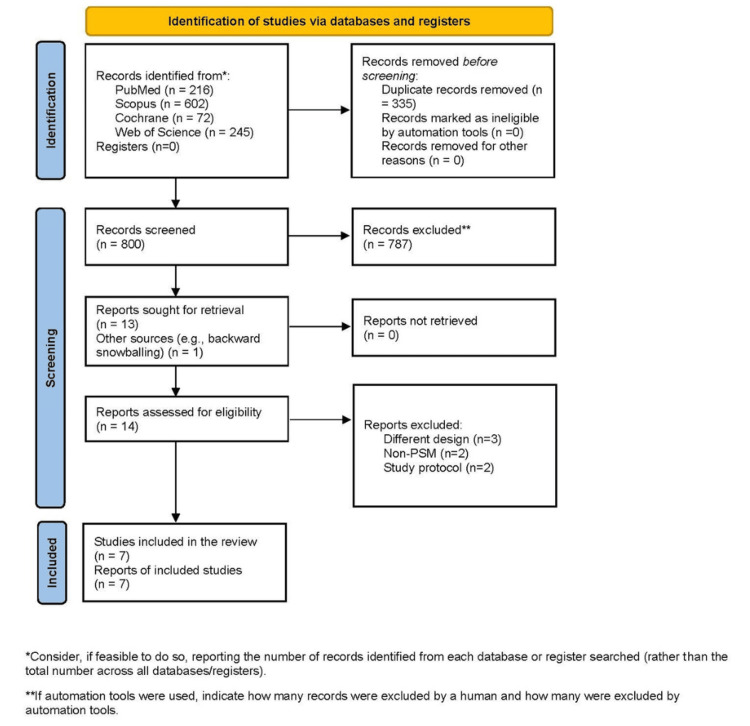
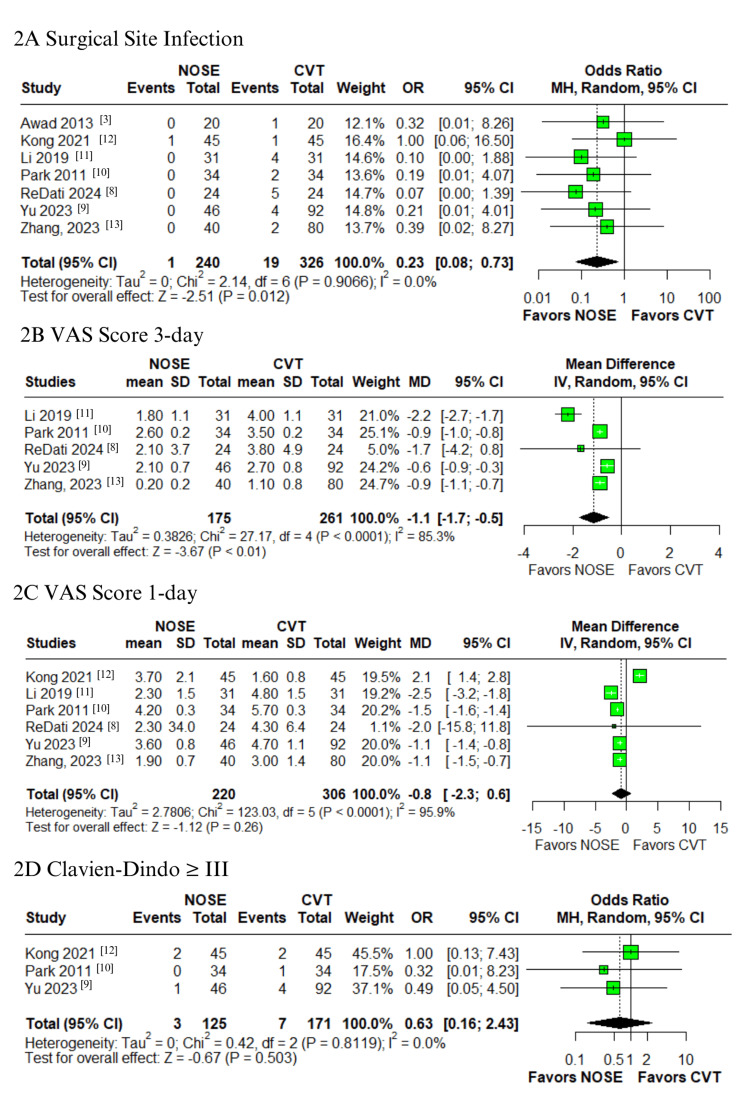
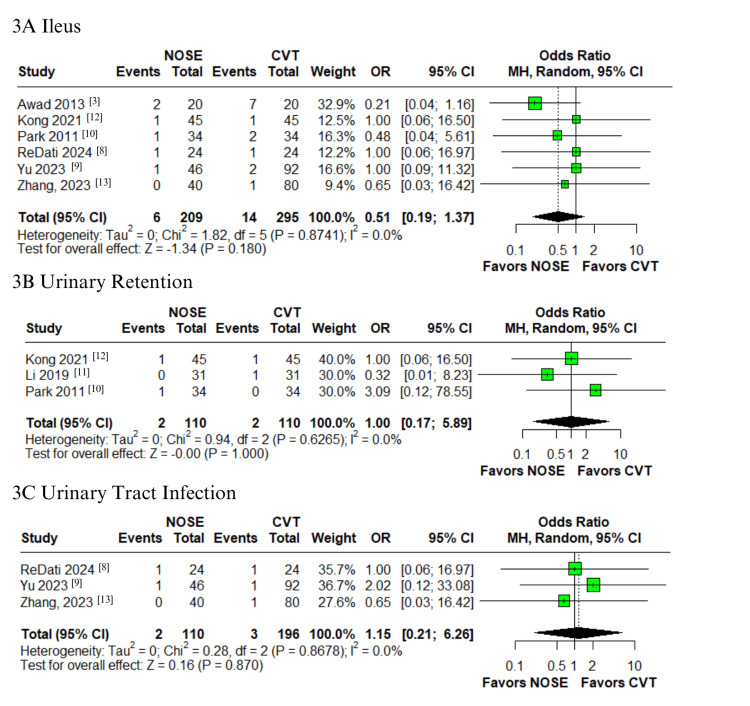
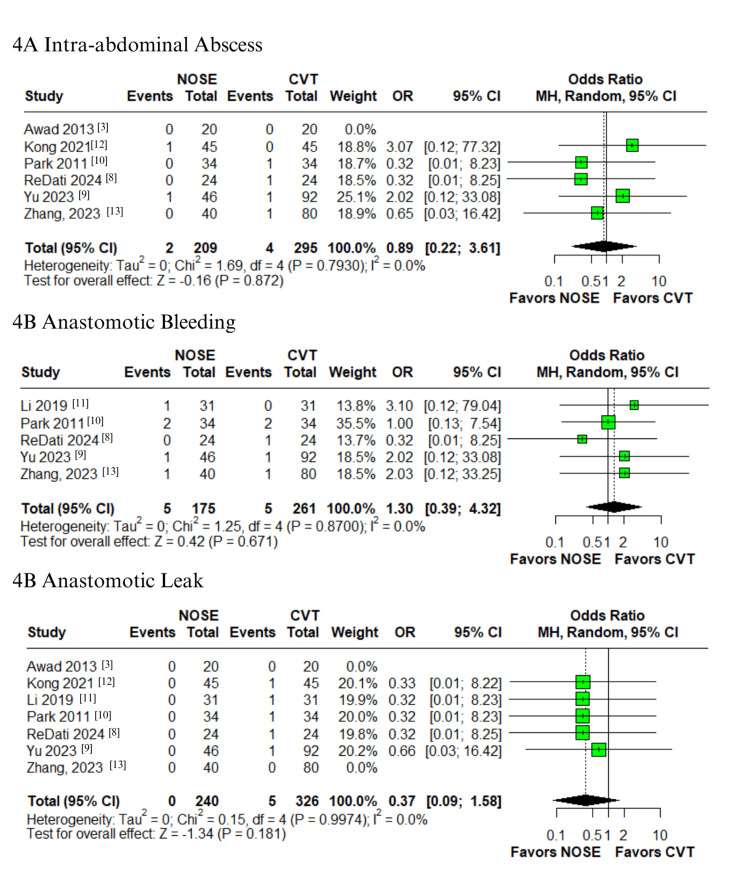
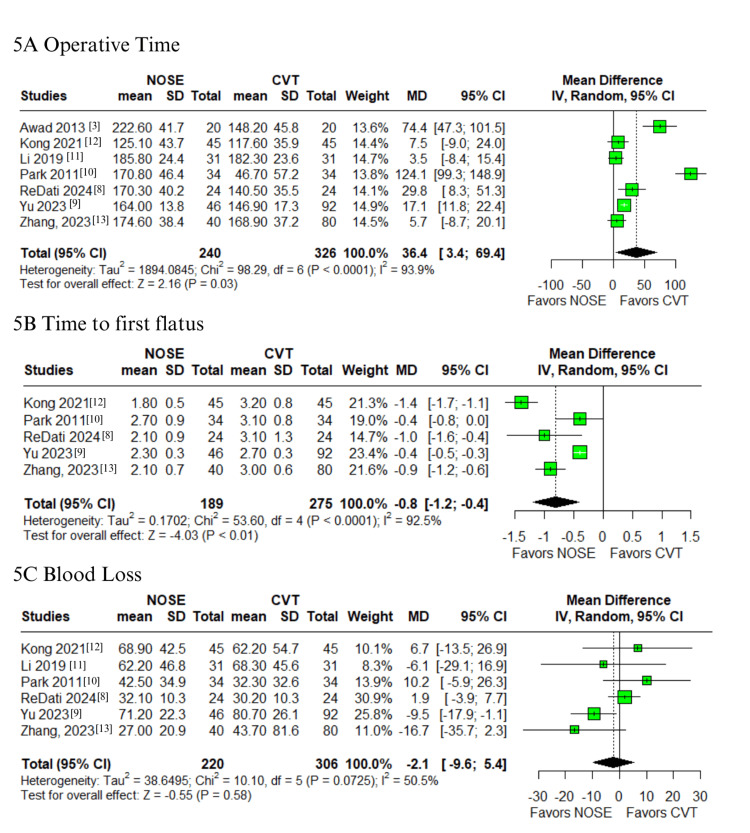
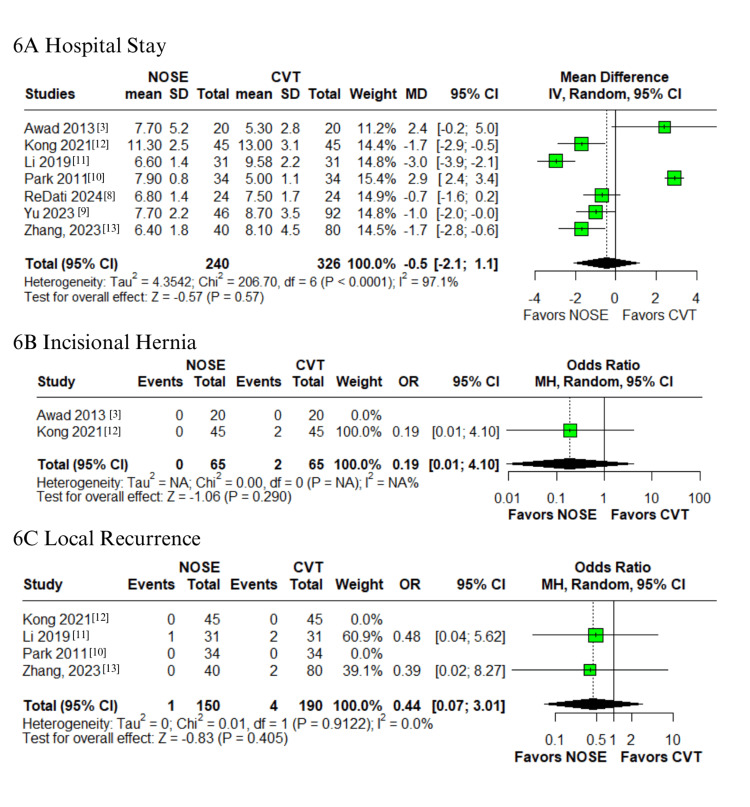
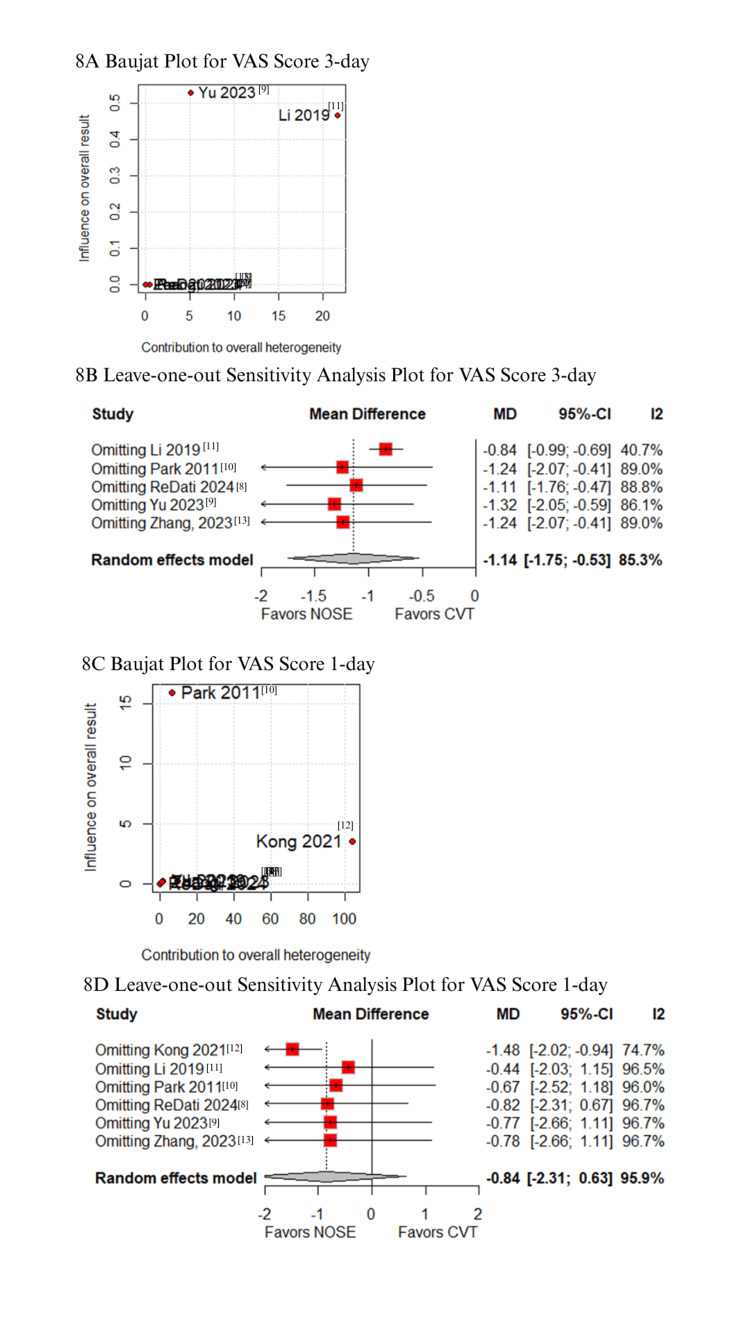
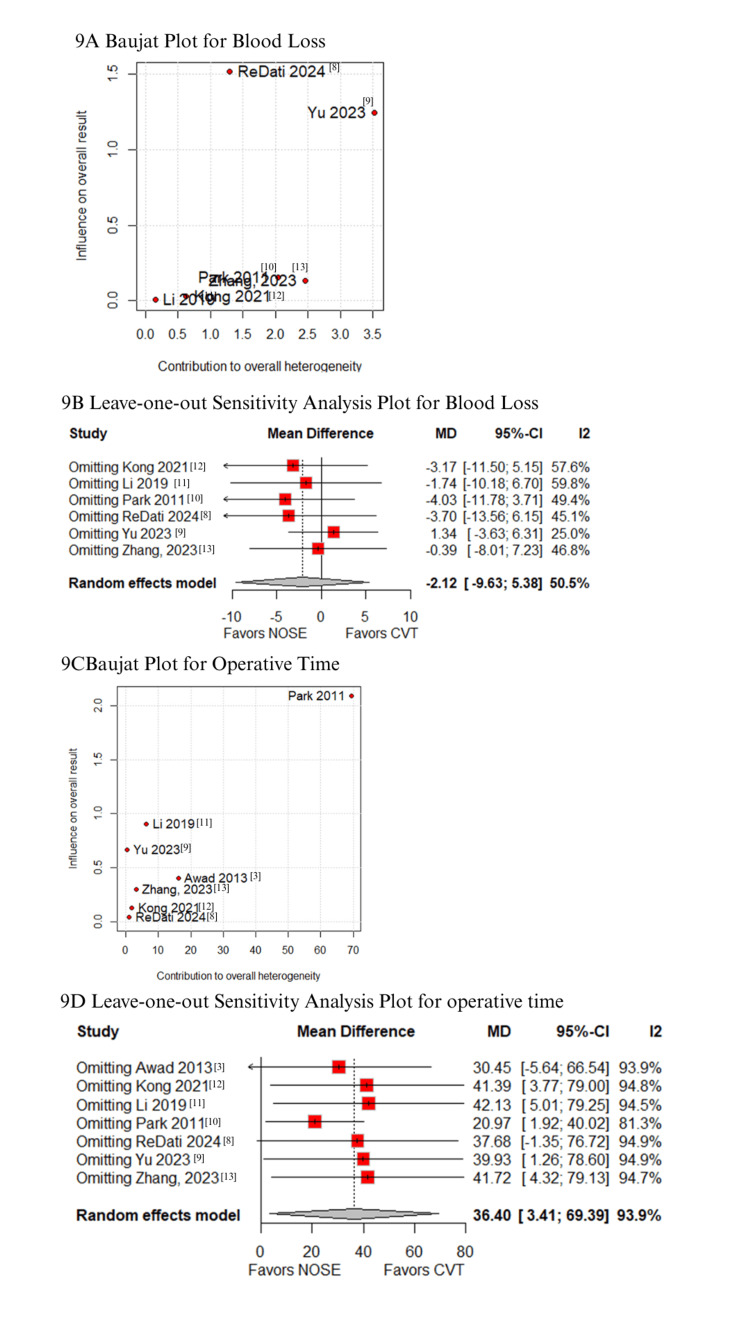
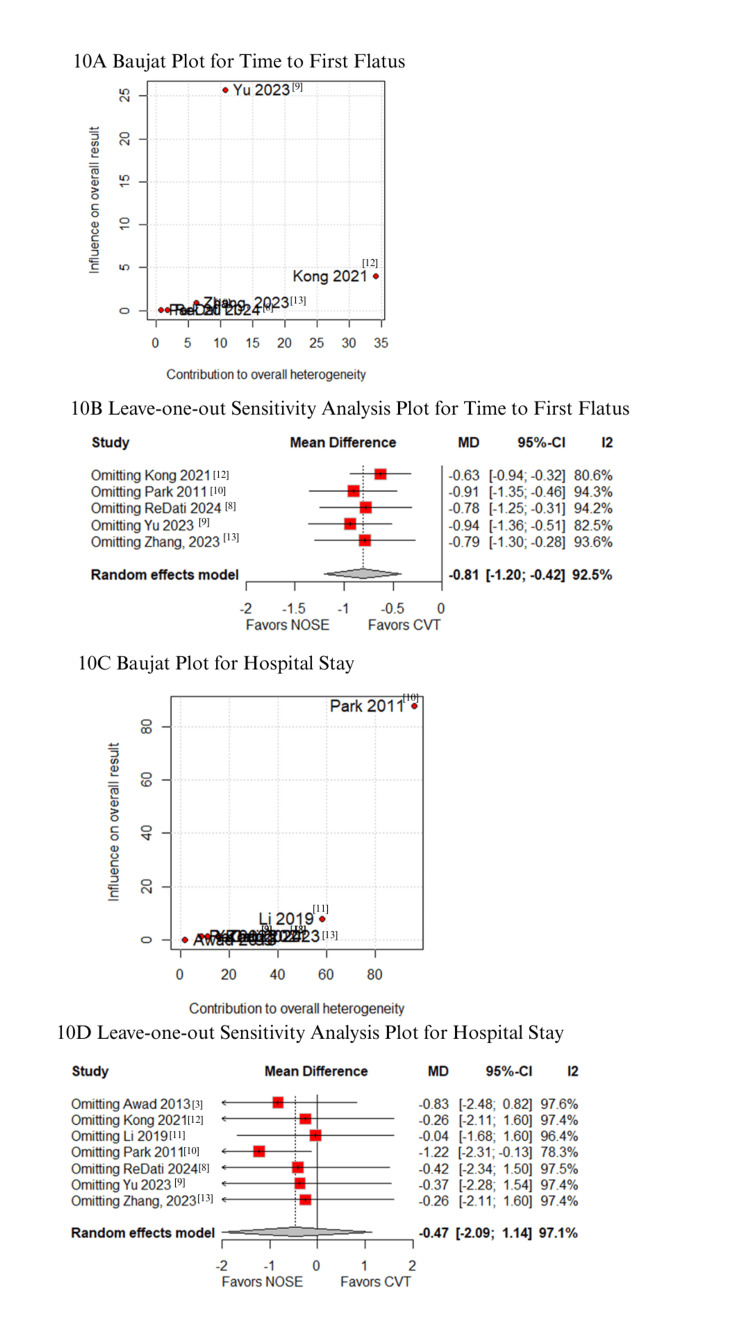
Minimally invasive surgery is the standard approach for right-sided colon cancer, but conventional laparoscopic specimen extraction (CVT) requires additional abdominal incisions, increasing the risk of postoperative complications and delayed recovery. Natural orifice specimen extraction (NOSE) minimizes abdominal incisions, potentially improving patient outcomes. This meta-analysis compares NOSE and CVT in terms of postoperative complications, operative characteristics, and long-term outcomes. A comprehensive literature search was conducted in PubMed, Scopus, the Cochrane Central Register of Clinical Trials, and Web of Science for studies available up to December 2024. A random-effects model was applied to compute ORs and mean differences (MDs) with 95% CIs. Heterogeneity was evaluated using the I² statistic. All statistical analyses were performed using R software (version 4.4.1, R Foundation for Statistical Computing). Seven propensity score-matched studies with 566 patients were included, with 240 (42.4%) undergoing NOSE and 326 (57.6%) undergoing CVT. NOSE was associated with significantly reduced postoperative pain on the 3rd day (MD -1.1; 95% CI -1.7 to -0.5; p < 0.01), lower SSI rates (OR 0.23; 95% CI 0.08-0.73; p = 0.012), and a shorter time to pass flatus (MD -0.8; 95% CI -1.2 to -0.4; p < 0.01). However, NOSE was linked to longer operative times (MD 36.4 minutes; 95% CI 3.4-69.4; p = 0.03). No significant differences were found in hospital stay (MD -0.5 days; 95% CI -2.1 to 1.1; p = 0.57), blood loss (MD -2.1; 95% CI -9.6 to 5.4; p = 0.58), or local recurrence (OR 0.44; 95% CI 0.07-3.01; p = 0.405). In conclusion, NOSE offers advantages such as reduced postoperative pain, lower SSI rates, and faster bowel recovery, with prolonged operative time as its main limitation. These findings support NOSE as a viable alternative to CVT for right-sided colon cancer without compromising safety or long-term outcomes.
Keywords: laparoscopic surgery; natural orifice specimen extraction; postoperative outcomes; propensity score matching; right-sided colon cancer.
Copyright © 2025, Pompeu et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Argilés G, Tabernero J, Labianca R, et al. Ann Oncol. 2020;31:1291–1305. - PubMed
-
- Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. CA Cancer J Clin. 2021;71:209–249. - PubMed
-
- Laparoscopic right hemicolectomy: a comparison of natural orifice versus transabdominal specimen extraction. Awad ZT, Griffin R. Surg Endosc. 2014;28:2871–2876. - PubMed
-
- Transrectal natural orifice specimen extraction (NOSE) with oncological safety: a prospective and randomized trial. Zhou ZQ, Wang K, Du T, et al. J Surg Res. 2020;254:16–22. - PubMed
-
- Clinical outcomes of laparoscopic-assisted natural orifice specimen extraction colectomy using a Cai tube for left-sided colon cancer: a prospective randomized trial. Xu SZ, Ding ZJ, Zhang SF, et al. Surg Endosc. 2023;37:749–758. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous