

Breast Cancer Brain Metastases: A Neurosurgical Point of View From a Single-Center Experience
- PMID: 40376375
- PMCID: PMC12080738
- DOI: 10.7759/cureus.82306
Breast Cancer Brain Metastases: A Neurosurgical Point of View From a Single-Center Experience
Abstract
Background: Brain metastases represent an important factor in breast cancer morbidity and mortality. Although various therapeutic options improved these patients' outcomes, the incidence of this disease is still rising. Several molecular subtypes of breast cancer have been studied, and human epidermal growth factor receptor 2 (HER2) positive and triple-negative breast cancer (TNBC) are more frequently associated with brain metastases. Therefore, anti-HER2 agents have been developed and studied, and they have shown promising results. Nevertheless, in patients with breast cancer brain metastases and acute neurological aggravation, neurosurgery is the primary option and the only one that can immediately reverse the symptoms. In the long run, a multimodal approach involving neurosurgical intervention can positively impact the prognosis.
Material and methods: Patients with a confirmed diagnosis of brain metastases from breast cancer (BMBC) between January 2013 and December 2023 were retrospectively reviewed. All patients were newly diagnosed and treated in the 3rd Neurosurgical Department at the Clinical Emergency Hospital, "Bagdasar-Arseni" in Bucharest, Romania. Statistical analyses were carried out and interpreted accordingly.
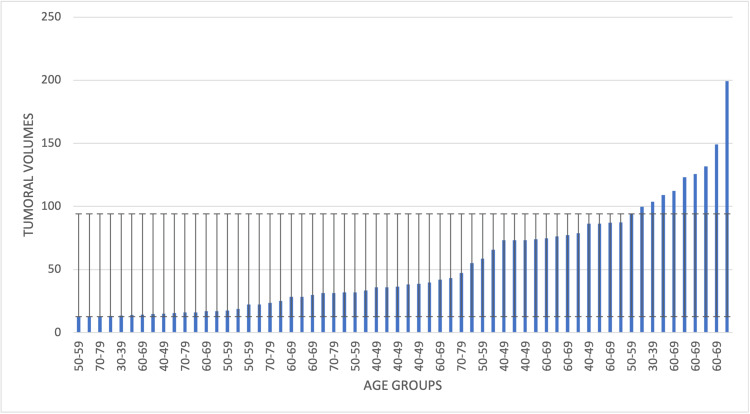
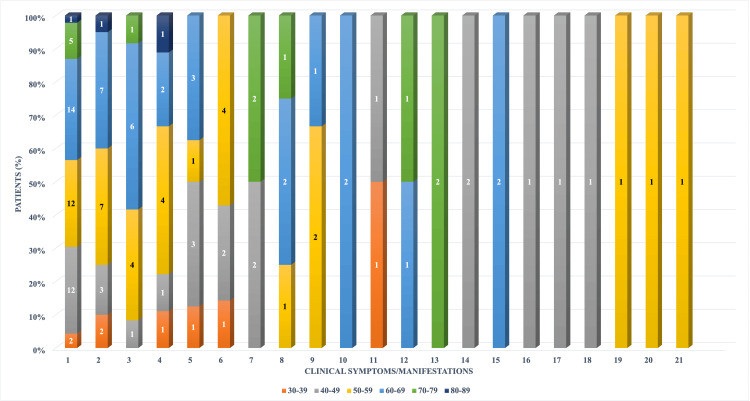
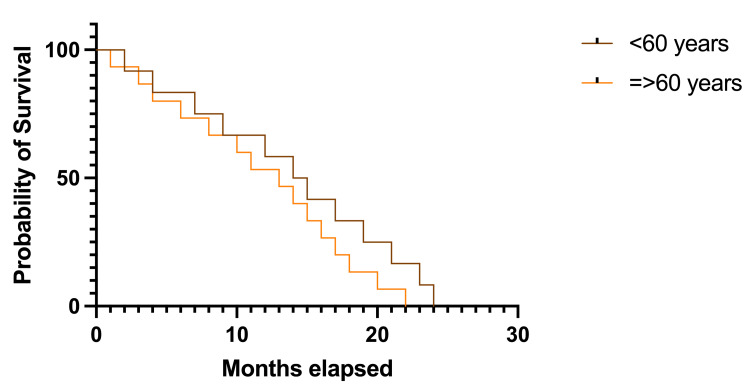
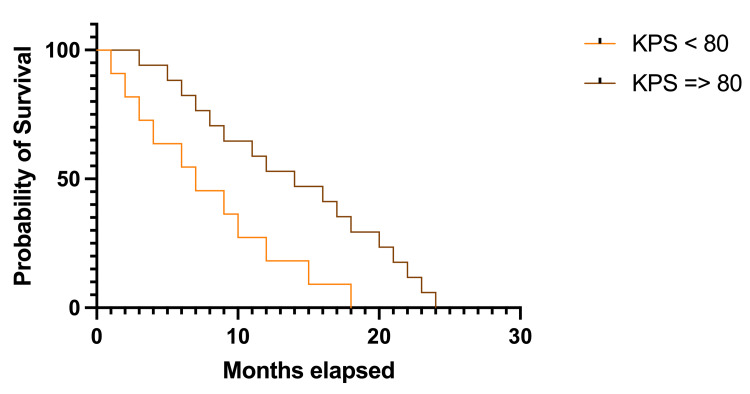
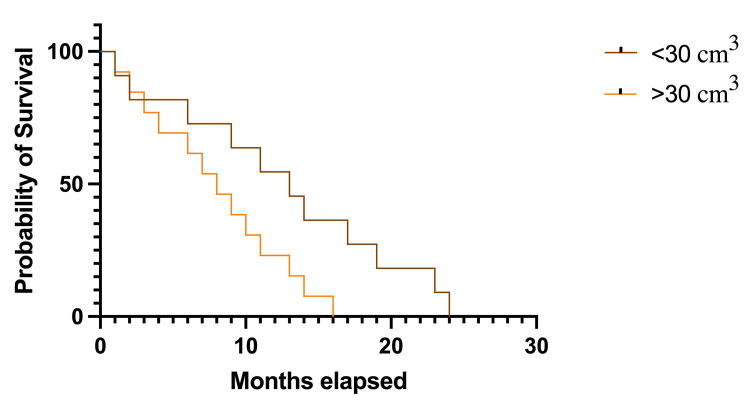
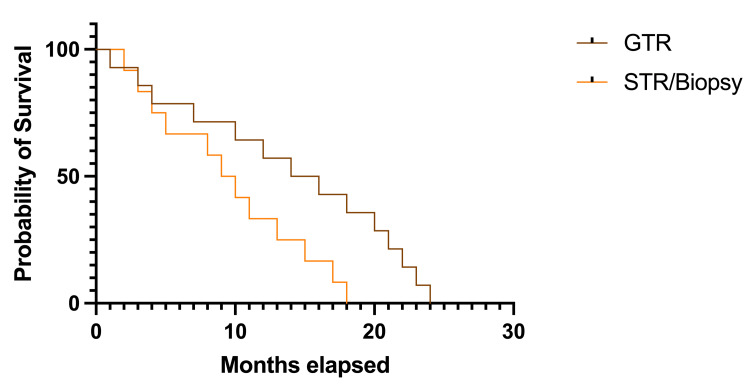
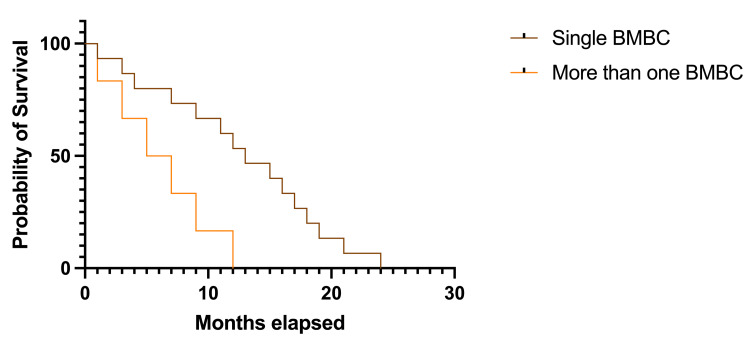
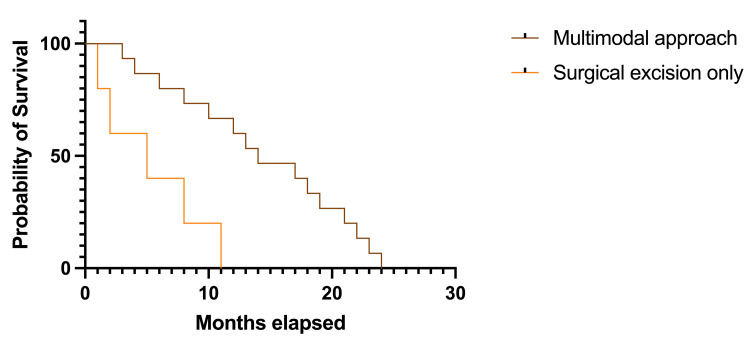
Results: The study analyzed 62 patients with BMBC. The median age at diagnosis was 57.19 years, and the most frequently encountered symptoms were represented by headaches, raised intracranial pressure syndrome, and motor deficits. More than 80% of the patients had a Karnofsky Performance Status (KPS) between 80 and 100, and the most associated comorbidities were cardiovascular and type 2 diabetes mellitus. A total of 88.70% of the patients had a single brain metastasis, and the most common localizations were the posterior fossa/cerebellum and frontal lobe. Gross-total resection was possible in 79.03% of the cases, while complications were recorded in 8.06%. Better survival rates were registered in patients of younger ages, with higher KPS, single BM, and smaller tumoral volumes, treated by gross-total resection and by a multimodal approach.
Conclusions: Notwithstanding significant advancements in the field of breast cancer, the prognosis of patients with brain metastases remains poor. However, a multimodal approach can prolong survival rates and improve outcomes, while in patients with acute clinical manifestations, neurosurgery remains the only immediate option to reverse the symptoms.
Keywords: brain metastases; breast cancer; multimodal approach; neurosurgery; outcomes.
Copyright © 2025, Tataranu et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Research Ethics Committee of the Clinical Emergency Hospital "Bagdasar-Arseni” issued approval 53407/04.11.2024. The study was conducted in accordance with the Declaration of Helsinki and approved by the Re-search Ethics Committee of the Clinical Emergency Hospital "Bagdasar-Arseni” (No. 53407/04.11.2024). Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Targeting brain metastases in breast cancer. Corti C, Antonarelli G, Criscitiello C, et al. Cancer Treat Rev. 2022;103:102324. - PubMed
-
- Brain metastases. Achrol AS, Rennert RC, Anders C, et al. Nat Rev Dis Primers. 2019;5:5. - PubMed
-
- Brain metastases from breast cancer. Santos J, Arantes J, Carneiro E, Ferreira D, Silva SM, Palma de Sousa S, Arantes M. Clin Neurol Neurosurg. 2020;197:106150. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous