

Efficacy of microsurgical denervation of the spermatic cord in patients with chronic scrotal pain following unsuccessful varicocelectomy
- PMID: 40376535
- PMCID: PMC12076242
- DOI: 10.21037/tau-2024-719
Efficacy of microsurgical denervation of the spermatic cord in patients with chronic scrotal pain following unsuccessful varicocelectomy
Abstract
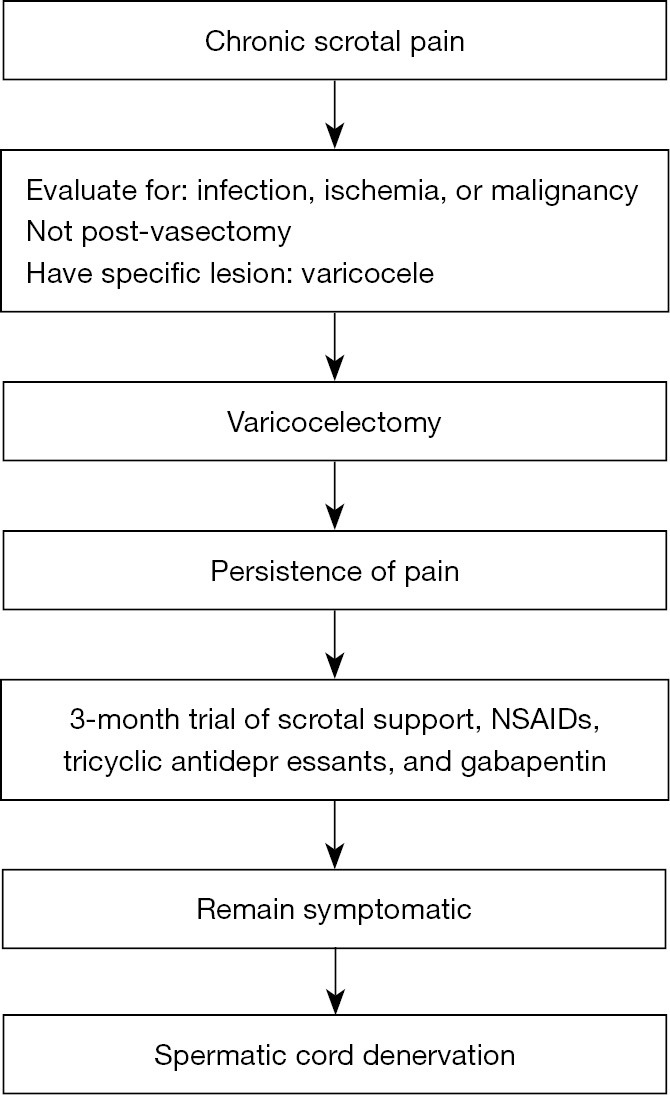
Background: Chronic scrotal pain (CSP) frequently persists following varicocelectomy, significantly impacting patients' quality of life and posing considerable therapeutic challenges. Recently, microsurgical denervation of the spermatic cord (MDSC) has emerged as a promising surgical alternative for managing CSP refractory to conventional varicocelectomy. This study evaluates the efficacy of MDSC as a treatment for CSP in patients who did not achieve symptomatic relief after varicocelectomy.
Methods: From March 2021 to March 2023, we conducted a retrospective cohort study of 45 male patients aged ≥18 years with persistent CSP following varicocelectomy. Inclusion criteria included patients unresponsive for more than three months post-varicocelectomy to medical treatments, including nonsteroidal anti-inflammatory drugs (NSAIDs), antidepressants, and anticonvulsants, and who demonstrated significant pain reduction following a spermatic cord block (SCB). Pain was assessed using the Numeric Rating Scale (NRS), a self-reported tool ranging from 0 to 10. All patients underwent MDSC based on their positive response to SCB.
Results: The average follow-up period was 14.0 months. Participants experienced significant pain reduction, with mean NRS pain scores decreasing from 7.5 pre-treatment to 1.7 following the SCB, and slightly rising to 1.8 post-operation. Significant pain relief, defined as a reduction of more than 50% in NRS score, was observed in 84.4% of cases. Minimal complications were reported, including one instance of surgical site infection, one case of postoperative bleeding, and two occurrences of numbness and burning sensations.
Conclusions: MDSC is a safe and effective option for the management of CSP in patients unresponsive to varicocelectomy, providing substantial pain relief with minimal complications.
Keywords: Microsurgical denervation of the spermatic cord (MDSC); chronic scrotal pain (CSP); varicocelectomy.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tau.amegroups.com/article/view/10.21037/tau-2024-719/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- Ciftci H, Savas M, Yeni E, et al. Chronic orchialgia and associated diseases. Current Urology 2010;4:67-70. 10.1159/000253415 - DOI