

Efficacy of pharmacological therapies in reducing outflow tract obstruction in patients with obstructive hypertrophic cardiomyopathy: a systematic review and meta-analysis
- PMID: 40377024
- PMCID: PMC12343041
- DOI: 10.1093/ehjcvp/pvaf036
Efficacy of pharmacological therapies in reducing outflow tract obstruction in patients with obstructive hypertrophic cardiomyopathy: a systematic review and meta-analysis
Abstract
Aims: Significant advancements have been made in the management of obstructive hypertrophic cardiomyopathy (oHCM), yet the extent of left ventricular outflow tract (LVOT) gradient reduction achieved with commonly used pharmacological therapies [beta-blockers (BBs), calcium channel blockers (CCBs), disopyramide, and cardiac myosin inhibitors (CMIs)] relative to each other is still unclear.
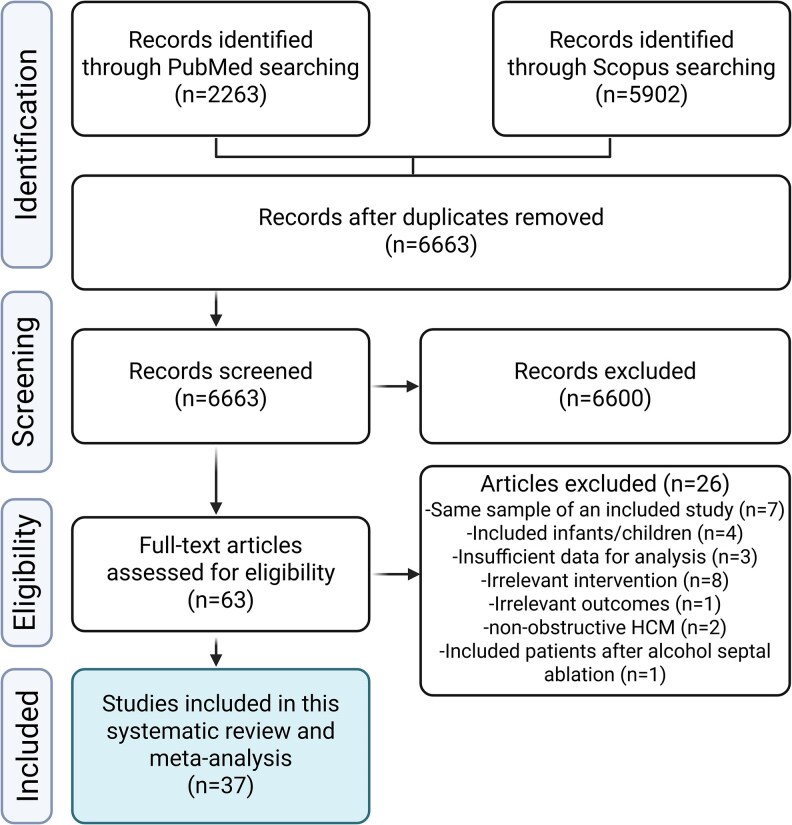
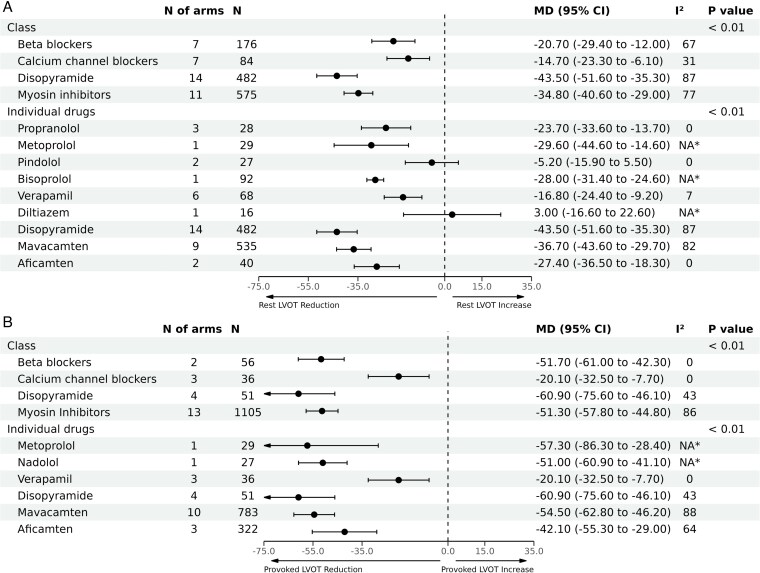
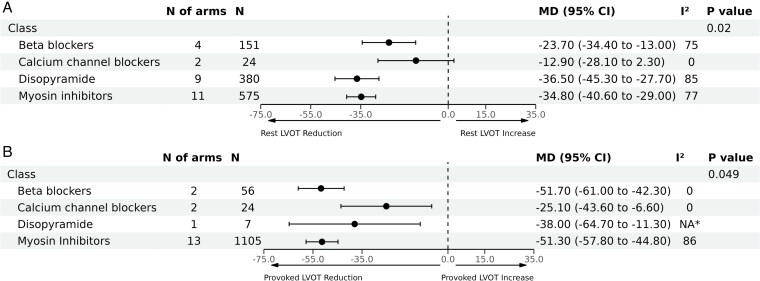
Methods and results: PubMed and Scopus were searched up to September 2024. Clinical trials or observational studies that assessed the changes associated with BBs, CCBs, disopyramide, or CMIs in LVOT gradient at rest or with provocation in patients with oHCM were included. Mean changes in LVOT gradients were pooled as mean differences (MD) with 95% confidence intervals (CIs) in a random-effects model. Thirty-seven studies, with 44 arms and 1898 patients, were included in the analysis. At the therapeutic class level, pooled analysis showed that disopyramide was associated with the highest reduction in LVOT gradient at rest [MD: -43.5 (95% CI, -51.6 to -35.3)], followed by CMIs [MD: -34.8 (95% CI, -40.6 to -29.0)], BBs [MD: -20.7 (95% CI, -29.4 to -12.0)], and then CCBs [MD: -14.7 (95% CI, -23.3 to -6.1)], inter-action P < 0.01. Within CMIs, mavacamten had a higher effect than aficamten on gradient reduction; among the included BBs, metoprolol showed the highest gradient reduction, while among CCBs, verapamil was the most effective (inter-action P < 0.01). Similar results were observed for provocable LVOT gradients.
Conclusion: Pharmacological therapies effectively reduced LVOT gradients in oHCM patients to varying degrees, with disopyramide and CMIs showing the highest effect, followed by BBs and CCBs.
Keywords: Hypertrophic cardiomyopathy; Left ventricular outflow tract obstruction; Medical treatment.
© The Author(s) 2025. Published by Oxford University Press on behalf of European Society of Cardiology.
Conflict of interest statement
Conflict of interest: none declared.
Figures
Similar articles
-
Concomitant Aficamten and Disopyramide in Symptomatic Obstructive Hypertrophic Cardiomyopathy.JACC Heart Fail. 2025 Apr 2:102441. doi: 10.1016/j.jchf.2025.03.008. Online ahead of print. JACC Heart Fail. 2025. PMID: 40285763
-
Efficacy and Safety of Mavacamten in the Treatment of Hypertrophic Cardiomyopathy: A Systematic Review.Heart Lung Circ. 2023 Sep;32(9):1049-1056. doi: 10.1016/j.hlc.2023.05.019. Epub 2023 Jul 14. Heart Lung Circ. 2023. PMID: 37453852
-
Calcium channel blockers for inhibiting preterm labour and birth.Cochrane Database Syst Rev. 2014 Jun 5;2014(6):CD002255. doi: 10.1002/14651858.CD002255.pub2. Cochrane Database Syst Rev. 2014. PMID: 24901312 Free PMC article.
-
Long-acting inhaled therapy (beta-agonists, anticholinergics and steroids) for COPD: a network meta-analysis.Cochrane Database Syst Rev. 2014 Mar 26;2014(3):CD010844. doi: 10.1002/14651858.CD010844.pub2. Cochrane Database Syst Rev. 2014. PMID: 24671923 Free PMC article.
-
Calcium channel blockers for primary and secondary Raynaud's phenomenon.Cochrane Database Syst Rev. 2017 Dec 13;12(12):CD000467. doi: 10.1002/14651858.CD000467.pub2. Cochrane Database Syst Rev. 2017. PMID: 29237099 Free PMC article.
Cited by
-
Our knowledge about atrial fibrillation steadily increases.Eur Heart J Cardiovasc Pharmacother. 2025 Aug 12;11(5):397-398. doi: 10.1093/ehjcvp/pvaf050. Eur Heart J Cardiovasc Pharmacother. 2025. PMID: 40796150 Free PMC article. No abstract available.
References
-
- Ommen SR, Mital S, Burke MA, Day SM, Deswal A, Elliott P, Evanovich LL, Hung J, Joglar JA, Kantor P, Kimmelstiel C, Kittleson M, Link MS, Maron MS, Martinez MW, Miyake CY, Schaff HV, Semsarian C, Sorajja P. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J Am Coll Cardiol 2020;76:e159–e240. - PubMed
-
- Ommen SR, Ho CY, Asif IM, Balaji S, Burke MA, Day SM, Dearani JA, Epps KC, Evanovich L, Ferrari VA, Joglar JA, Khan SS, Kim JJ, Kittleson MM, Krittanawong C, Martinez MW, Mital S, Naidu SS, Saberi S, Semsarian C, Times S, Waldman CB. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American Heart Association/American College of Cardiology joint committee on clinical practice guidelines. Circulation 2024;149:e1239–e1311. - PubMed
-
- Ayoub C, Geske JB, Larsen CM, Scott CG, Klarich KW, Pellikka PA. Comparison of valsalva maneuver, amyl nitrite, and exercise echocardiography to demonstrate latent left ventricular outflow obstruction in hypertrophic cardiomyopathy. Am J Cardiol 2017;120:2265–2271. - PubMed
-
- Geske JB, Cullen MW, Sorajja P, Ommen SR, Nishimura RA. Assessment of left ventricular outflow gradient: hypertrophic cardiomyopathy versus aortic valvular stenosis. JACC Cardiovasc Interv 2012;5:675–681. - PubMed
LinkOut - more resources
Full Text Sources
