

Changing metastatic patterns associate with dynamics of circulating tumor DNA in metastatic castration-resistant prostate cancer
- PMID: 40377440
- PMCID: PMC12082820
- DOI: 10.1093/oncolo/oyaf107
Changing metastatic patterns associate with dynamics of circulating tumor DNA in metastatic castration-resistant prostate cancer
Abstract
Background: Circulating tumor DNA (ctDNA) acts as an early biomarker of the efficacy of androgen receptor signaling inhibitor (ARSI) therapy. In this study, we aimed to reveal if ctDNA can supplement imaging to better predict metastasis burden and radiographic progression disease (PD) in metastatic castration-resistant prostate cancer (mCRPC).
Methods: Targeted next-generation sequencing was performed to assess ctDNA fraction. Radiographic evidence was documented by conventional imaging according to Prostate Cancer Working Group 3 criteria.
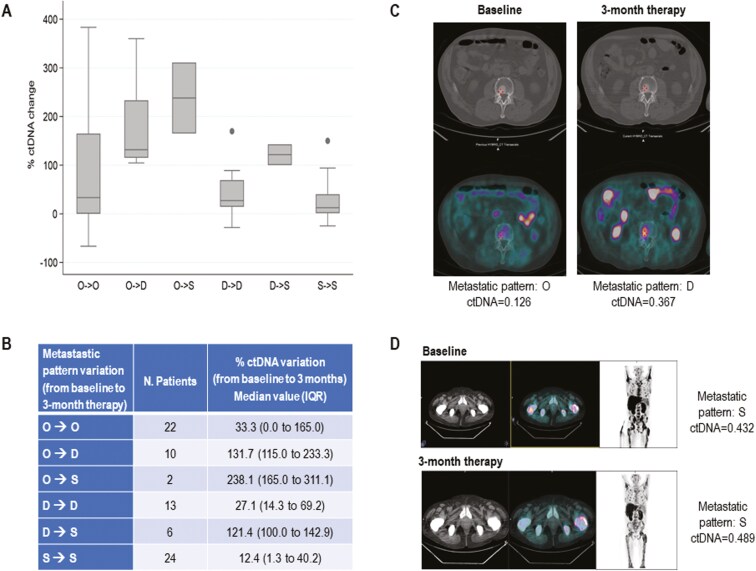
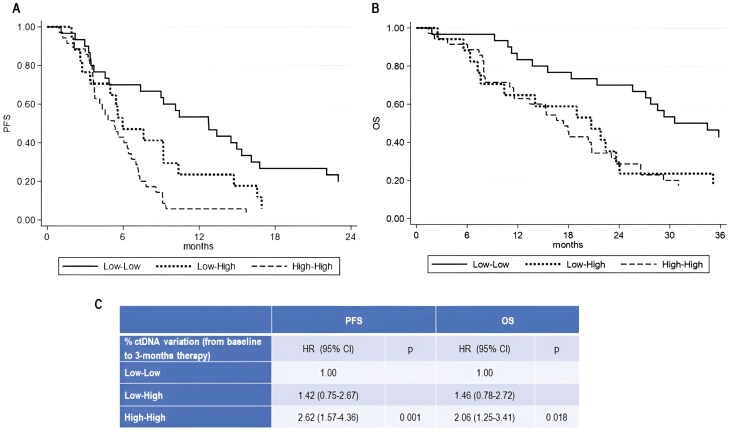
Results: We prospectively collected plasma samples from 112 mCRPC with bone (n = 77), lymph nodal (n = 31), and visceral (n = 4) metastases. Only bone metastatic patterns were significantly associated with median ctDNA at baseline, during treatment and at PD (P <.0001). At first radiographic restaging, 24 (31.2%) men with a progressive worsening of bone disease had early ctDNA rise with a % ctDNA variation of 150.6% (interquartile range [IQR] = 104.9-210.7] compared with 11.1% (IQR = 0-36.6), P <.0001, in men with no change in bone disease. Univariate analysis showed that early ctDNA rise was significantly associated with progression free/overall survival (PFS/OS). In multivariable analysis including ctDNA change from baseline to 3-month treatment, variation of bone metastatic patterns (from oligometastatic to polymetastatic and/or to widespread disease), presence of visceral metastasis, age, PSA, performance status and prior docetaxel therapy, the transition from low- to high-ctDNA within 3 months of starting ARSI therapy was a significant predictor of OS (HR = 2.50, 90% CI, 1.06-5.88, P =.035) and persistent high level of ctDNA was a predictor of PFS (HR = 2.53, 95% CI, 1.10-5.81, P =.028). Metastatic involvement demonstrated that the transition from bone polymetastatic to widespread disease and the presence of visceral metastases were both associated with worse OS (HR = 2.43, 95% CI, 1.10-5.35, P =.028, and HR = 3.40, 95% CI, 1.50-7.66, P =.003, respectively). Prior therapy with docetaxel represented an independent predictor of both PFS and OS (HR = 2.47, 95% CI, 1.40-4.35, P =.002, and HR = 1.78, 95% CI, 1.00-3.15, P =.049, respectively).
Conclusions: Early ctDNA variation might reflect changes in metastatic burden and, likely, in bone metastatic patterns on ARSI therapy allowing to track pattern of disease progression and to predict outcome.
Keywords: androgen receptor signaling inhibitors; bone metastasis; ctDNA; mCRPC; metastatic pattern.
© The Author(s) 2025. Published by Oxford University Press.
Conflict of interest statement
V.C. has served as a consultant/advisory board member for Johnson&Johnson, Astellas, Merck, AstraZeneca, Amgen, EISAI, Recordati, Novartis, Ipsen, and Bayer and has received speaker honoraria or travel support from Astellas, Johnson&Johnson, Ipsen, Bayer, Gilead, and BristolMyers Squibb. G.S. reports honoraria from Bayer, BMS, and Ipsen. N.B. reports travel support from Ipsen, Novartis, Johnson&Johnson, Pfizer, and Advanced Accelerator Applications, speaker honoraria from BMS. Novartis. C.L. reports honoraria for advisory boards or speaker fees from Ipsen, BMS, and MSD. M.C.C. reports travel accommodation from Ipsen. U.D.G. reports honoraria for advisory boards or speaker fees from Pfizer, BMS, MSD, PharmaMar, Astellas, Bayer, Ipsen, Roche, Novartis, Clovis, GSK, AstraZeneca, institutional research grants from AstraZeneca, Sanofi, and Roche. No potential conflicts of interest were disclosed by the other authors.
Figures
Similar articles
-
Plasma Cell-free DNA Concentration and Outcomes from Taxane Therapy in Metastatic Castration-resistant Prostate Cancer from Two Phase III Trials (FIRSTANA and PROSELICA).Eur Urol. 2018 Sep;74(3):283-291. doi: 10.1016/j.eururo.2018.02.013. Epub 2018 Feb 28. Eur Urol. 2018. PMID: 29500065 Free PMC article. Clinical Trial.
-
Prognostic Value of Low-Pass Whole Genome Sequencing of Circulating Tumor DNA in Metastatic Castration-Resistant Prostate Cancer.Clin Chem. 2023 Apr 3;69(4):386-398. doi: 10.1093/clinchem/hvac224. Clin Chem. 2023. PMID: 36762756
-
Deep targeted sequencing of circulating tumor DNA to inform treatment in patients with metastatic castration-resistant prostate cancer.J Exp Clin Cancer Res. 2025 Apr 14;44(1):120. doi: 10.1186/s13046-025-03356-0. J Exp Clin Cancer Res. 2025. PMID: 40229848 Free PMC article.
-
Therapeutic biomarkers in metastatic castration-resistant prostate cancer: does the state matter?Crit Rev Clin Lab Sci. 2024 May;61(3):178-204. doi: 10.1080/10408363.2023.2266482. Epub 2023 Oct 26. Crit Rev Clin Lab Sci. 2024. PMID: 37882463 Review.
-
Predicting therapy response and resistance in metastatic prostate cancer with circulating tumor DNA.Urol Oncol. 2018 Aug;36(8):380-384. doi: 10.1016/j.urolonc.2017.11.017. Epub 2017 Dec 14. Urol Oncol. 2018. PMID: 29248429 Review.
References
-
- Bray F, Laversanne M, Sung H, et al.Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229-263. https://doi.org/10.3322/caac.21834 - DOI - PubMed
-
- Davies A, Conteduca V, Zoubeidi A, Beltran H.. Biological evolution of castration-resistant prostate cancer. Eur Urol Focus. 2019;5:147-154. https://doi.org/10.1016/j.euf.2019.01.016 - DOI - PubMed
-
- Halabi S, Kelly WK, Ma H, et al.Meta-analysis evaluating the impact of site of metastasis on overall survival in men with castration-resistant prostate cancer. J Clin Oncol. 2016;34:1652-1659. https://doi.org/10.1200/JCO.2015.65.7270 - DOI - PMC - PubMed
-
- Bubendorf L, Schöpfer A, Wagner U, et al.Metastatic patterns of prostate cancer: an autopsy study of 1,589 patients. Hum Pathol. 2000;31:578-583. https://doi.org/10.1053/hp.2000.6698 - DOI - PubMed
-
- Scher HI, Morris MJ, Stadler WM, et al.; Prostate Cancer Clinical Trials Working Group 3. Trial design and objectives for castration-resistant prostate cancer: updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J Clin Oncol. 2016;34:1402-1418. https://doi.org/10.1200/JCO.2015.64.2702 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
