

Current Management of Pulmonary Hydatid Cyst
- PMID: 40377486
- PMCID: PMC12036369
- DOI: 10.5152/eurasianjmed.2025.24761
Current Management of Pulmonary Hydatid Cyst
Abstract
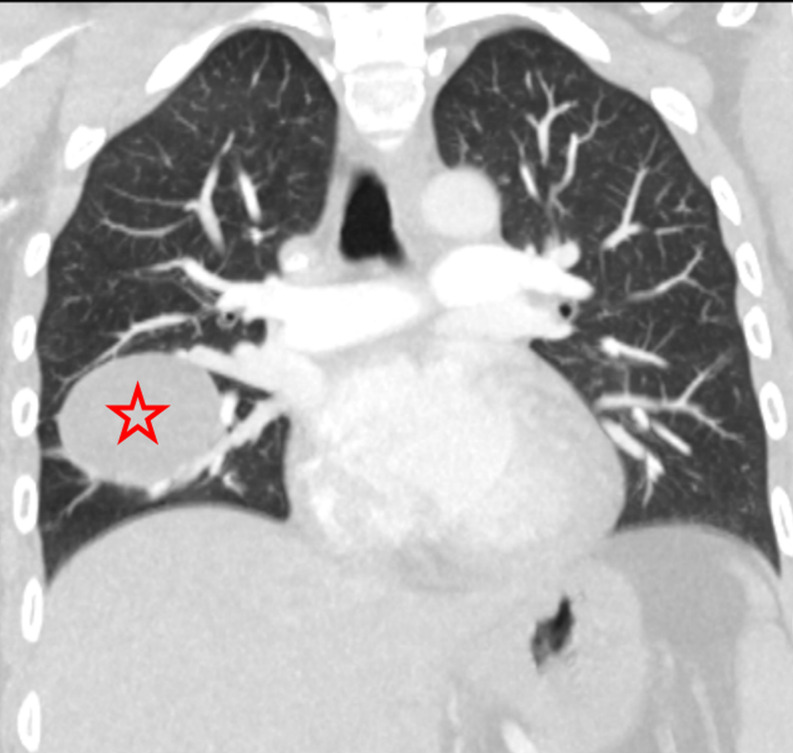
Hydatid disease is a zoonotic infection caused by the larval stage of the Echinococcus granulosus worm, commonly found in developing countries. The lungs represent the second most commonly affected organ in both children and adults. The disease is more common in children than in adults, and the growth of hydatid cysts is more rapid in children than in adults. Diagnosing uncomplicated cases of hydatid cysts is generally straightforward clinically and radiologically. However, difficulties may arise in diagnosing complicated cysts. Surgery is the definitive treatment for pulmonary hydatid cysts. The surgical approach is contingent upon a number of factors, including the dimensions of the cyst, the integrity of its structure, whether it is solitary or multiple, unilateral or bilateral, and the extent of lung parenchyma destruction. In contrast to the liver, surgical treatment is promptly planned upon the diagnosis of a pulmonary hydatid cyst. The most effective surgical method is cystotomy and capitonnage while maintaining the integrity of the lung parenchyma to the greatest extent possible. Albendazole is the preferred medical treatment, but it is not recommended for intact cysts during the preoperative period due to its potential to weaken the cyst wall and cause rupture. Albendazole is administered to prevent postoperative recurrence and for treatment in cases where surgery is not feasible.
Conflict of interest statement
Figures





References
-
- Aydin Y, Ulas AB, Ince I, et al. Large case series analysis of cystic echinococcosis. Indian J Surg. 2021;83(suppl 4):897 906. ( 10.1007/s12262-021-03061-0) - DOI
-
- Acosta-Jamett G, Hernández FA, Castro N, et al. Prevalence rate and risk factors of human cystic echinococcosis: a cross-sectional, community-based, abdominal ultrasound study in rural and urban north-central Chile. PLoS Negl Trop Dis. 2022;16(3):e0010280. ( 10.1371/journal.pntd.0010280) - DOI - PMC - PubMed
-
- Tamarozzi F, Akhan O, Cretu CM, et al. Epidemiological factors associated with human cystic echinococcosis: a semi-structured questionnaire from a large population-based ultrasound cross-sectional study in eastern Europe and Turkey. Parasit Vectors. 2019;12(1):371. ( 10.1186/s13071-019-3634-1) - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources