

Reproducibility and reliability of flow quantification using CMR 2D-phase contrast and 4D-Flow in secondary mitral valve regurgitation
- PMID: 40377789
- PMCID: PMC12241284
- DOI: 10.1007/s10554-025-03421-x
Reproducibility and reliability of flow quantification using CMR 2D-phase contrast and 4D-Flow in secondary mitral valve regurgitation
Abstract
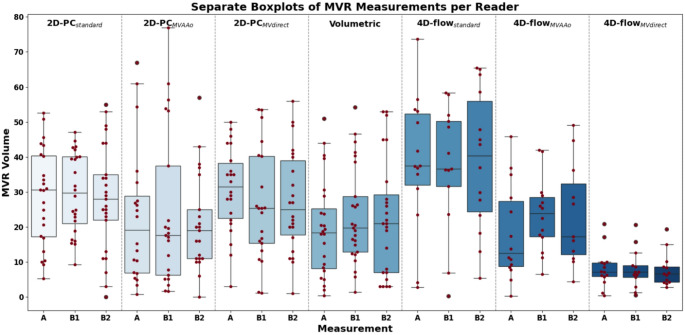
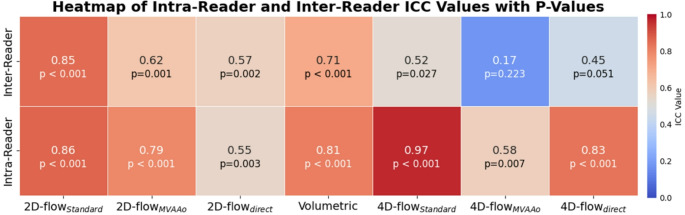
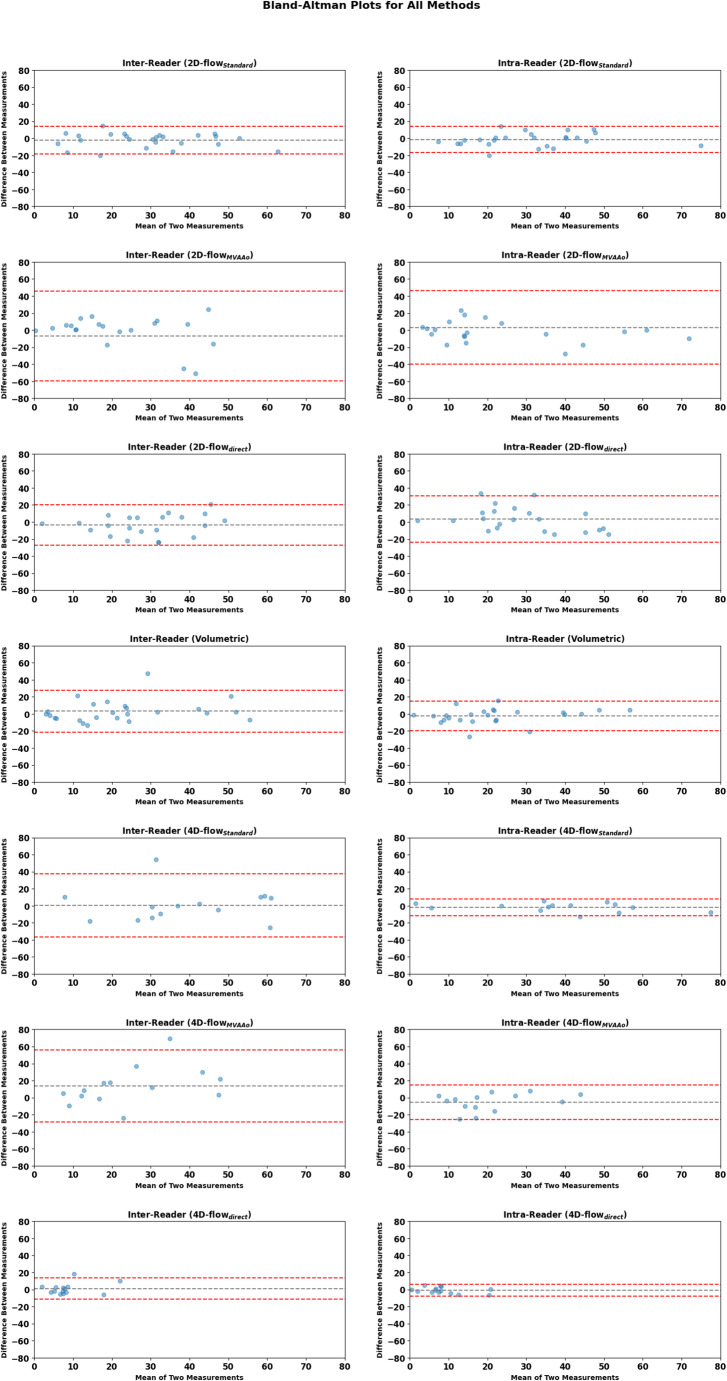
Accurate quantification of mitral valve regurgitation (MVR) is crucial for patient management. While different MVR quantification methods based on cardiac magnetic resonance imaging (CMR) exist, their reproducibility and reliability remain uncertain. This study aims to evaluate the reproducibility of different CMR 2D-phase contrast (PC) and 4D-flow MVR quantification methods. The inter-reader and intra-reader reproducibility were assessed using intraclass correlation coefficients (ICC). Seven methods were evaluated: 2D-PC standard (LVSV minus aortic flow), 2D-PC mitral-aortic (mitral inflow minus aortic flow), 2D-PC direct (quantifying mitral backflow), 4D-flow standard, 4D-flow mitral-aortic, 4D-flow direct, and volumetric method (LVSV minus RVSV) in 32 patients (74.8 ± 9.8 years, 28% females) with secondary MVR, analyzed independently by two experienced readers. A total of 26 patients were included in the analysis for 2D-PC and 15 for 4D-flow methods. Among all techniques, 2D-PC standard was the most reliable method with both good inter-reader (ICC = 0.85, p < 0.001) and intra-reader agreement (ICC = 0.87, p < 0.001). The 4D-flow standard (ICC = 0.97, p < 0.001) and the volumetric method (ICC = 0.81, p < 0.001) showed excellent and good intra-reader agreements, respectively, but only moderate inter-reader reproducibility (ICC = 0.52, p = 0.027 and ICC = 0.71, p < 0.001). In patients with secondary MVR, 2D-PC standard method demonstrated the highest reproducibility, while 4D-flow methods showed excellent intra-reader reliability but more variable inter-reader agreement. Standardized post-processing protocols and training would likely enhance the clinical application of these techniques. Future studies should investigate these methods in larger, diverse cohorts and correlate findings with clinical outcomes.
Keywords: 2D-PC; 4D-flow; Cardiovascular; Challenges; Data analysis; Flow; Heart; Validation; Valves; Velocity & flow.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This study was conducted in compliance with the ethical guidelines outlined in the Declaration of Helsinki. Ethical approval was obtained from the local ethics committee (KEK-BE 2021 − 00704), as stated in the manuscript. Written informed consent was obtained from all participants prior to their inclusion in the study. Competing interests: Prof. Dr. Christoph Gräni is an author on this manuscript and also serves as the Editor-in-Chief of The International Journal of Cardiovascular Imaging. To ensure an unbiased review process, we understand this submission will be handled by Associate Editors. Prof. Gräni also received funding from the SNSF, InnoSuisse, the Center for Artificial Intelligence in Medicine (CAIM) at the University of Bern, the GAMBIT Foundation, the Novartis Foundation for Medical-Biological Research, and the Swiss Heart Foundation, all unrelated to the scope of this submitted work. The other authors declare no competing interests.
Figures


Similar articles
-
Free-breathing single-beat exercise cardiovascular magnetic resonance with generative artificial intelligence for evaluation of volumetric and functional cardiac indices: A reproducibility study.J Cardiovasc Magn Reson. 2025 Summer;27(1):101901. doi: 10.1016/j.jocmr.2025.101901. Epub 2025 Apr 30. J Cardiovasc Magn Reson. 2025. PMID: 40316174 Free PMC article.
-
Direct mitral regurgitation quantification in hypertrophic cardiomyopathy using 4D flow CMR jet tracking: evaluation in comparison to conventional CMR.J Cardiovasc Magn Reson. 2021 Dec 6;23(1):138. doi: 10.1186/s12968-021-00828-y. J Cardiovasc Magn Reson. 2021. PMID: 34865629 Free PMC article.
-
Robustness of 4D flow MRI derived aortic wall shear stress and pulse wave velocity across different protocols in healthy controls and in patients with bicuspid aortic valve.Int J Cardiovasc Imaging. 2025 Jan;41(1):137-149. doi: 10.1007/s10554-024-03299-1. Epub 2024 Dec 9. Int J Cardiovasc Imaging. 2025. PMID: 39652207 Free PMC article.
-
Quantitation of mitral regurgitation with cardiac magnetic resonance imaging: a systematic review.Heart. 2016 Dec 1;102(23):1864-1870. doi: 10.1136/heartjnl-2015-309054. Epub 2016 Oct 12. Heart. 2016. PMID: 27733535
-
Mitral valve regurgitation assessed by intraventricular CMR 4D-flow: a systematic review on the technological aspects and potential clinical applications.Int J Cardiovasc Imaging. 2023 Oct;39(10):1963-1977. doi: 10.1007/s10554-023-02893-z. Epub 2023 Jun 16. Int J Cardiovasc Imaging. 2023. PMID: 37322317 Free PMC article. Review.
References
-
- Boudoulas KD, Borer JS, Boudoulas H (2013) Etiology of valvular heart disease in the 21st century. Cardiology 126:139–152. 10.1159/000354221 - PubMed
-
- Asgar AW, Mack MJ, Stone GW (2015) Secondary mitral regurgitation in heart failure. J Am Coll Cardiol 65:1231–1248. 10.1016/j.jacc.2015.02.009 - PubMed
-
- Obadia J-F, Messika-Zeitoun D, Leurent G, Iung B, Bonnet G, Piriou N et al (2018) Percutaneous repair or medical treatment for secondary mitral regurgitation. N Engl J Med 379:2297–2306. 10.1056/NEJMoa1805374 - PubMed
-
- Stone GW, Lindenfeld J, Abraham WT, Kar S, Lim DS, Mishell JM et al (2018) Transcatheter Mitral-Valve repair in patients with heart failure. N Engl J Med 379:2307–2318. 10.1056/NEJMoa1806640 - PubMed
-
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, Gentile F et al 2020 ACC/AHA guideline for the management of patients with valvular heart disease: A report of the American college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation 2021;143. 10.1161/CIR.0000000000000923 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
