

Sleep architecture and dementia risk in adults: an analysis of 5 cohorts from the Sleep and Dementia Consortium
- PMID: 40377976
- PMCID: PMC12417016
- DOI: 10.1093/sleep/zsaf129
Sleep architecture and dementia risk in adults: an analysis of 5 cohorts from the Sleep and Dementia Consortium
Abstract
Study objectives: Poor sleep may play a role in the risk of dementia. However, few studies have investigated the association between polysomnography (PSG)-derived sleep architecture and dementia incidence. We examined the relationship between sleep architecture and dementia incidence across five US-based cohort studies from the Sleep and Dementia Consortium.
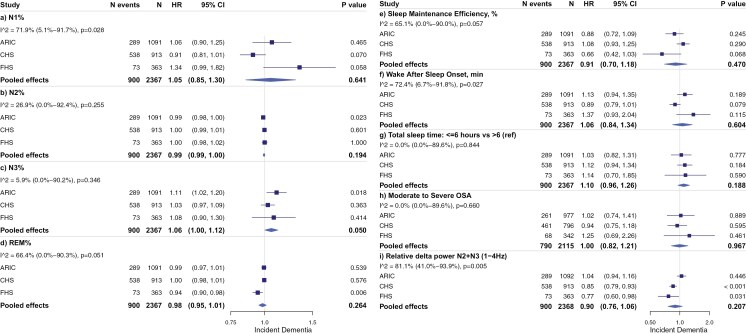
Methods: Percent of time spent in stages of sleep (N1, N2, N3, rapid eye movement sleep), wake after sleep onset, sleep maintenance efficiency, apnea-hypopnea index, and relative delta power were derived from a single night home-based PSG. Dementia was ascertained in each cohort using its cohort-specific criteria. Each cohort performed Cox proportional hazard regressions for each sleep exposure and incident dementia, adjusting for age, sex, body mass index, antidepressant use, sedative use, and APOE e4 status. Results were then pooled in a random effects model.
Results: The pooled sample comprised 4657 participants (30% women) aged ≥ 60 years (mean age was 74 years at sleep assessment). There were 998 (21.4%) dementia cases (median follow-up time of 5 to 19 years). Pooled effects of the five cohorts showed no association between sleep architecture and incident dementia. When pooled analysis was restricted to the three cohorts which had dementia case ascertainment based on DSM-IV/V criteria (n = 2374), higher N3% was marginally associated with an increased risk of dementia (hazard ratio (HR): 1.06; 95%CI: 1.00-1.12, per percent increase N3, p = .050).
Conclusions: There were no consistent associations between sleep architecture measured and the risk of incident dementia. Implementing more nuanced sleep metrics and examination of associations with dementia subtypes remains an important next step for uncovering more about sleep-dementia associations.
Keywords: Alzheimer’s disease; dementia; sleep; sleep macro-architecture.
© The Author(s) 2025. Published by Oxford University Press on behalf of Sleep Research Society.
Figures


Update of
-
Sleep macro-architecture and dementia risk in adults: Meta-analysis of 5 cohorts from the Sleep and Dementia Consortium.medRxiv [Preprint]. 2024 Nov 5:2024.11.05.24316677. doi: 10.1101/2024.11.05.24316677. medRxiv. 2024. Update in: Sleep. 2025 Sep 9;48(9):zsaf129. doi: 10.1093/sleep/zsaf129. PMID: 39802761 Free PMC article. Updated. Preprint.
References
-
- Edwards BA, O’Driscoll DM, Ali A, Jordan AS, Trinder J, Malhotra A. Aging and sleep: physiology and pathophysiology. Semin Respir Crit Care Med. 2010;31(5):618–633. doi: https://doi.org/ 10.1055/s-0030-1265902 - DOI - PMC - PubMed
-
- Tononi G, Cirelli C. Sleep and synaptic homeostasis: a hypothesis. Brain Res Bull. 2003;62(2):143–150. doi: https://doi.org/ 10.1016/j.brainresbull.2003.09.004 - DOI - PubMed
-
- Wunderlin M, Zust MA, Feher KD, Kloppel S, Nissen C. The role of slow wave sleep in the development of dementia and its potential for preventative interventions. Psychiatry Res Neuroimaging. 2020;306:111178. doi: https://doi.org/ 10.1016/j.pscychresns.2020.111178 - DOI - PubMed
-
- Lucey BP, McCullough A, Landsness EC, et al. Reduced non-rapid eye movement sleep is associated with tau pathology in early Alzheimer’s disease. Sci Transl Med. 2019;11(474):eaau6550. doi: https://doi.org/ 10.1126/scitranslmed.aau6550 - DOI - PMC - PubMed
-
- Winer JR, Mander BA, Helfrich RF, et al. Sleep as a potential biomarker of tau and beta-amyloid burden in the human brain. J Neurosci. 2019;39(32):6315–6324. doi: https://doi.org/ 10.1523/JNEUROSCI.0503-19.2019 - DOI - PMC - PubMed
MeSH terms
Grants and funding
- N01 HC085080/HL/NHLBI NIH HHS/United States
- RF1 AG059421/AG/NIA NIH HHS/United States
- R01 AG027576/AG/NIA NIH HHS/United States
- 75N92022D00004/HL/NHLBI NIH HHS/United States
- R21 MD012738/MD/NIMHD NIH HHS/United States
- R35 AG071916/AG/NIA NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- R01 NS017950/NS/NINDS NIH HHS/United States
- UF1 NS125513/NS/NINDS NIH HHS/United States
- R01 AG054076/AG/NIA NIH HHS/United States
- R01 HL070848/HL/NHLBI NIH HHS/United States
- R01 AG015928/AG/NIA NIH HHS/United States
- 75N92022D00002/HL/NHLBI NIH HHS/United States
- R01 HL071194/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01 HC085082/HL/NHLBI NIH HHS/United States
- R01 HL070847/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- R01 HL146339/HL/NHLBI NIH HHS/United States
- R01 AG062531/AG/NIA NIH HHS/United States
- R01 AR035583/AR/NIAMS NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- R01 AG026720/AG/NIA NIH HHS/United States
- N01 HC085083/HL/NHLBI NIH HHS/United States
- R01 AR035584/AR/NIAMS NIH HHS/United States
- R01 AG070867/AG/NIA NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- R01 HL070842/HL/NHLBI NIH HHS/United States
- U01 AG042124/AG/NIA NIH HHS/United States
- U01 AG042145/AG/NIA NIH HHS/United States
- R01 AG049607/AG/NIA NIH HHS/United States
- R01 HL105756/HL/NHLBI NIH HHS/United States
- U01 HL064360/HL/NHLBI NIH HHS/United States
- R01 AG005407/AG/NIA NIH HHS/United States
- R01 AG066524/AG/NIA NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- K24 HL159246/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- U01 AG042168/AG/NIA NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- R01 HL070841/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- R01 HL070838/HL/NHLBI NIH HHS/United States
- P30 AG066546/AG/NIA NIH HHS/United States
- 75N92022D00003/HL/NHLBI NIH HHS/United States
- U01 HL053934/HL/NHLBI NIH HHS/United States
- 75N92021D00006/HL/NHLBI NIH HHS/United States
- 75N92022D00005/HL/NHLBI NIH HHS/United States
- 75N92019D00031/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- R01 AR035582/AR/NIAMS NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- R01 AG005394/AG/NIA NIH HHS/United States
- R01 HL070837/HL/NHLBI NIH HHS/United States
- 75N92022D00001/HL/NHLBI NIH HHS/United States
- U01 AG042143/AG/NIA NIH HHS/United States
- N01 HC085081/HL/NHLBI NIH HHS/United States
- U01 AG042139/AG/NIA NIH HHS/United States
- R01 AG027574/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
