

A Single-Arm Phase 2 Trial of Doxorubicin Plus Zalifrelimab (Anti-CTLA-4 Antibody) and Balstilimab (Anti-PD-1 Antibody) in Advanced/Metastatic Soft Tissue Sarcomas
- PMID: 40378054
- PMCID: PMC12260506
- DOI: 10.1158/1078-0432.CCR-25-0618
A Single-Arm Phase 2 Trial of Doxorubicin Plus Zalifrelimab (Anti-CTLA-4 Antibody) and Balstilimab (Anti-PD-1 Antibody) in Advanced/Metastatic Soft Tissue Sarcomas
Abstract
Purpose: Doxorubicin is standard chemotherapy for metastatic soft tissue sarcomas (STS) but also enhances innate/adaptive immune responses by inducing immunogenic cell death. Most STS are immune "cold" tumors that do not respond to immune checkpoint inhibitors (ICI) blocking PD-1 and cytotoxic T lymphocyte antigen-4. We hypothesized that concurrent doxorubicin would improve tumor immunogenicity and boost the efficacy of ICI in STS.
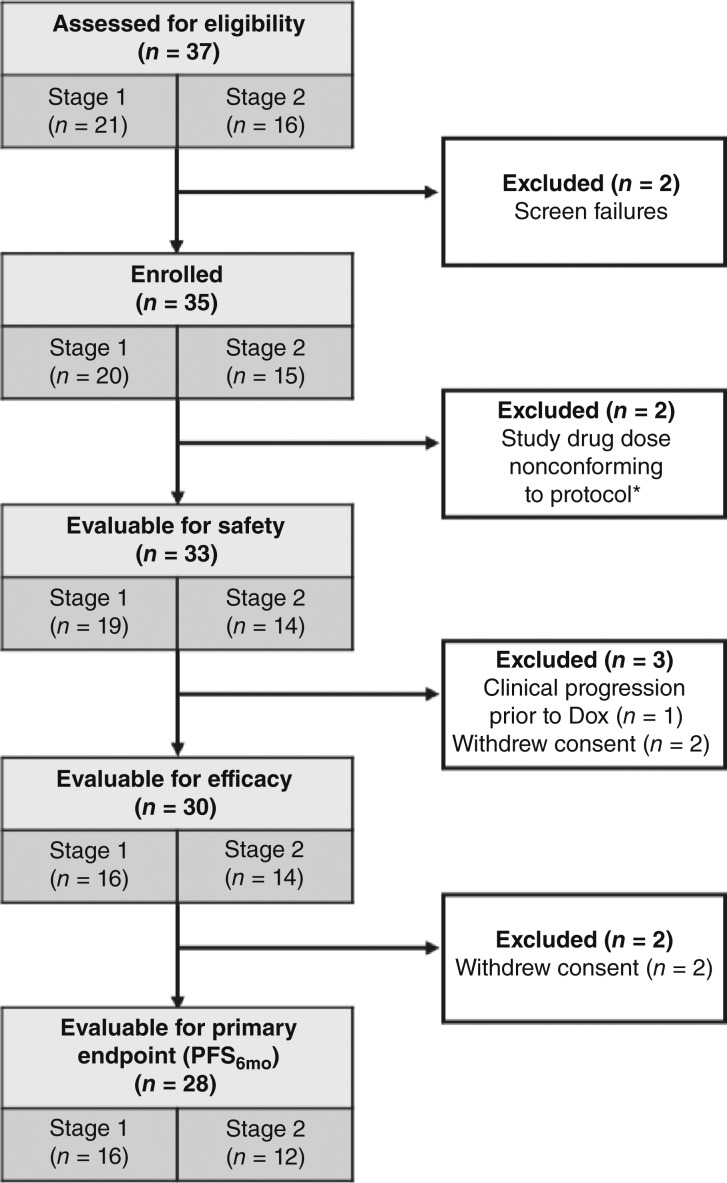
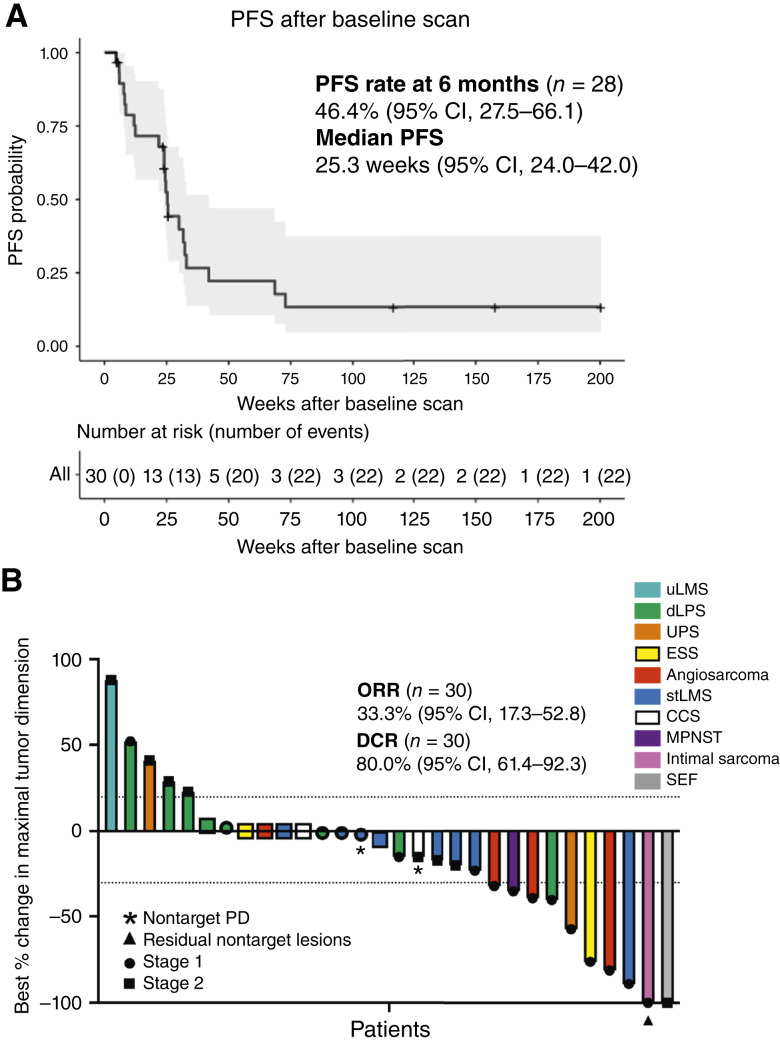
Patients and methods: We conducted a single-arm, phase 2 trial of doxorubicin plus zalifrelimab (anti-cytotoxic T lymphocyte antigen-4 antibody) and balstilimab (anti-PD-1 antibody) for patients with advanced/metastatic STS without prior doxorubicin or ICI (NCT04028063). The study was a Simon minimax two-stage design to accrue 28 patients evaluable for primary endpoint of progression-free survival rate at 6 months (PFS6mo) by RECIST 1.1. The study aimed to improve PFS6mo by 20% over a historic null rate of 43.4% with doxorubicin monotherapy. Secondary endpoints included the objective response rate, disease control rate, overall survival, duration of response, and adverse events (AE).
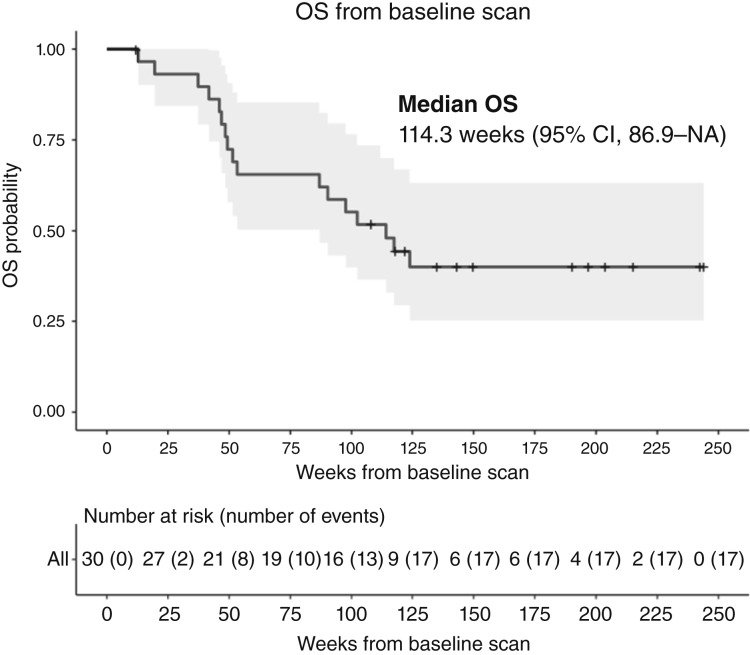
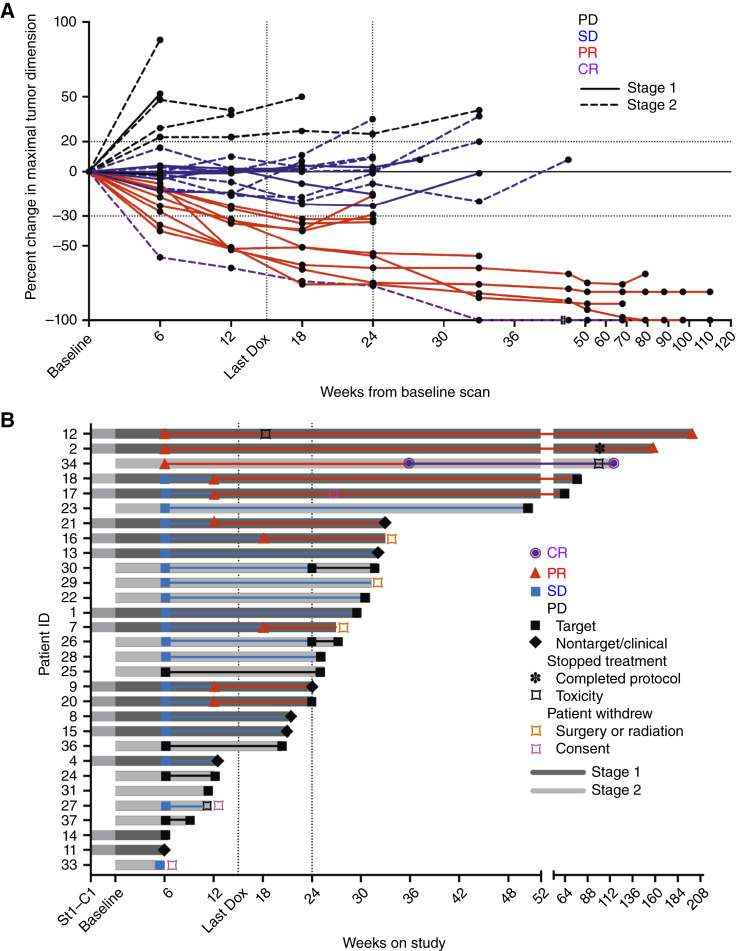
Results: The PFS6mo for 28 evaluable patients was 46.4% [95% confidence interval (CI), 27.5-66.1] and not superior to the null rate, with a median PFS of 25.3 weeks (95% CI, 24.0-42). The best objective response rate was 33.3% (95% CI, 17.3-52.8) with a disease control rate of 80.0% (95% CI, 61.4-92.3), including STS types unlikely to respond to doxorubicin or ICI alone. Grade 3/4 treatment-related AE occurred in 45% of patients, with immune-mediated AE requiring immunosuppression in 9%.
Conclusions: Although the study did not meet the predefined endpoint for PFS improvement, promising signals of efficacy warrant future investigation including response/resistance biomarkers to inform patient selection.
©2025 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
B.A. Wilky reports personal fees and other support from Agenus Inc. during the conduct of the study and personal fees from Springworks, Deciphera, Boehringer Ingelheim, AADI, and Inhibrx outside the submitted work. No disclosures were reported by the other authors.
Figures
References
-
- National Cancer Institute . SEER*Explorer: an interactive website for SEER cancer statistics [Internet]. Bethesda (MD): Surveillance Research Program, National Cancer Institute; 2023. Data source(s): SEER Incidence Data, November 2022 Submission (1975–2020), SEER 22 registries (excluding Illinois and Massachusetts). Expected Survival Life Tables by Socio-Economic Standards. [updated 2023 Nov 16; cited 2024 Sep 3]. Available from: https://seer.cancer.gov/statistics-network/explorer/.
-
- Wood GE, Meyer C, Petitprez F, D’Angelo SP. Immunotherapy in sarcoma: current data and promising strategies. Am Soc Clin Oncol Educ Book 2024;44:e432234. - PubMed
-
- Petitprez F, de Reyniès A, Keung EZ, Chen TWW, Sun CM, Calderaro J, et al. B cells are associated with survival and immunotherapy response in sarcoma. Nature 2020;577:556–60. - PubMed
-
- Italiano A, Bessede A, Pulido M, Bompas E, Piperno-Neumann S, Chevreau C, et al. Pembrolizumab in soft-tissue sarcomas with tertiary lymphoid structures: a phase 2 PEMBROSARC trial cohort. Nat Med 2022;28:1199–206. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
