

Application of imaging mass cytometry for spatially profiling the microenvironment of salivary glands in primary Sjögren's syndrome
- PMID: 40379615
- PMCID: PMC12084299
- DOI: 10.1038/s41419-025-07717-7
Application of imaging mass cytometry for spatially profiling the microenvironment of salivary glands in primary Sjögren's syndrome
Abstract
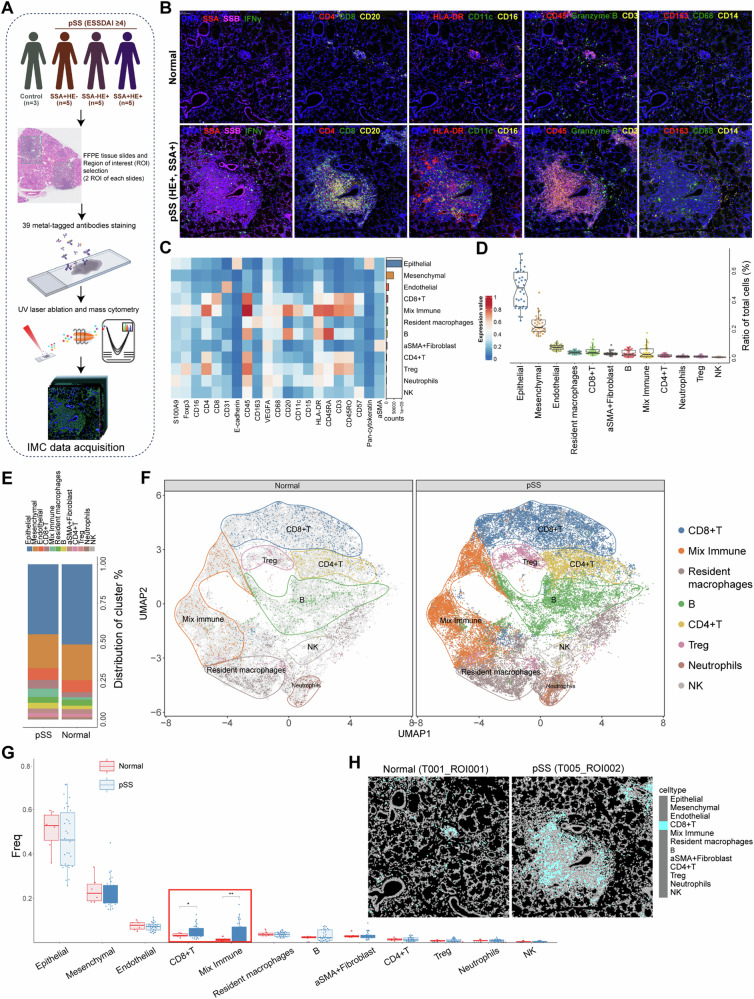
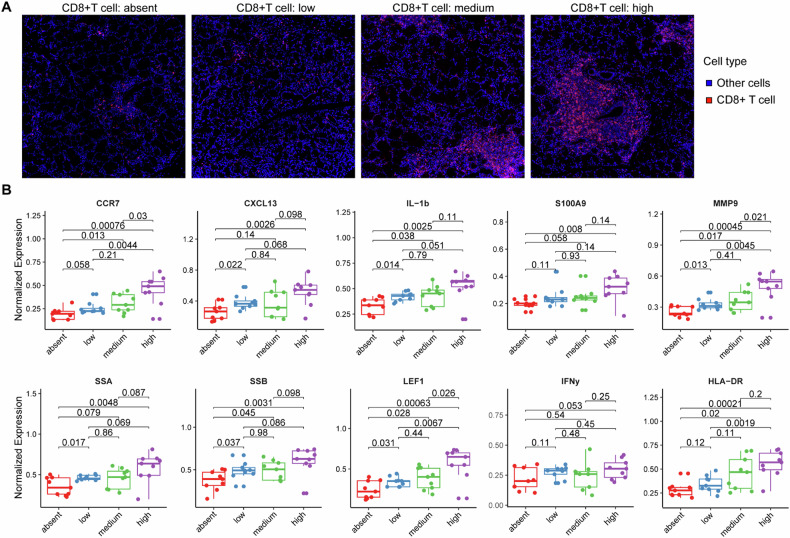
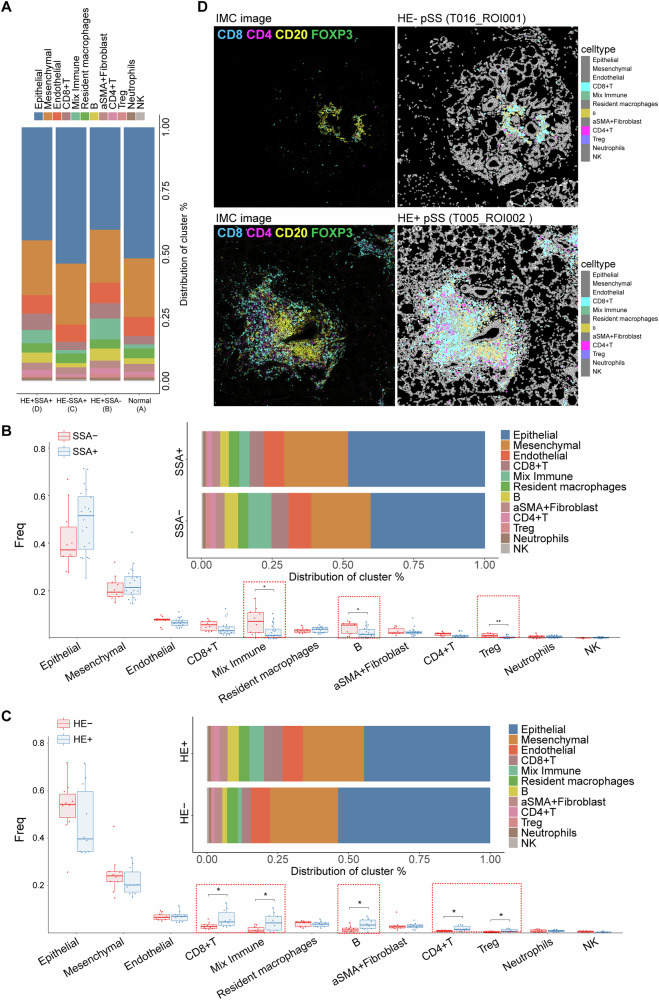
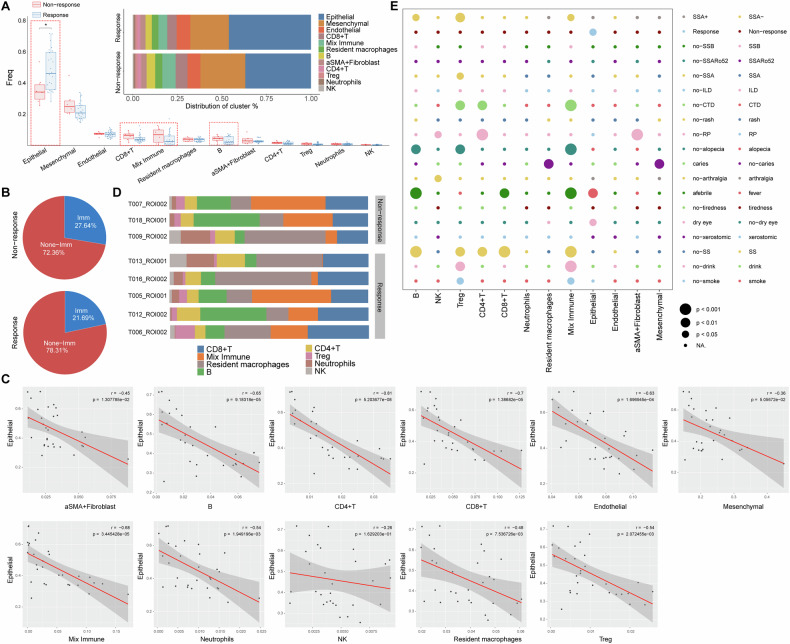
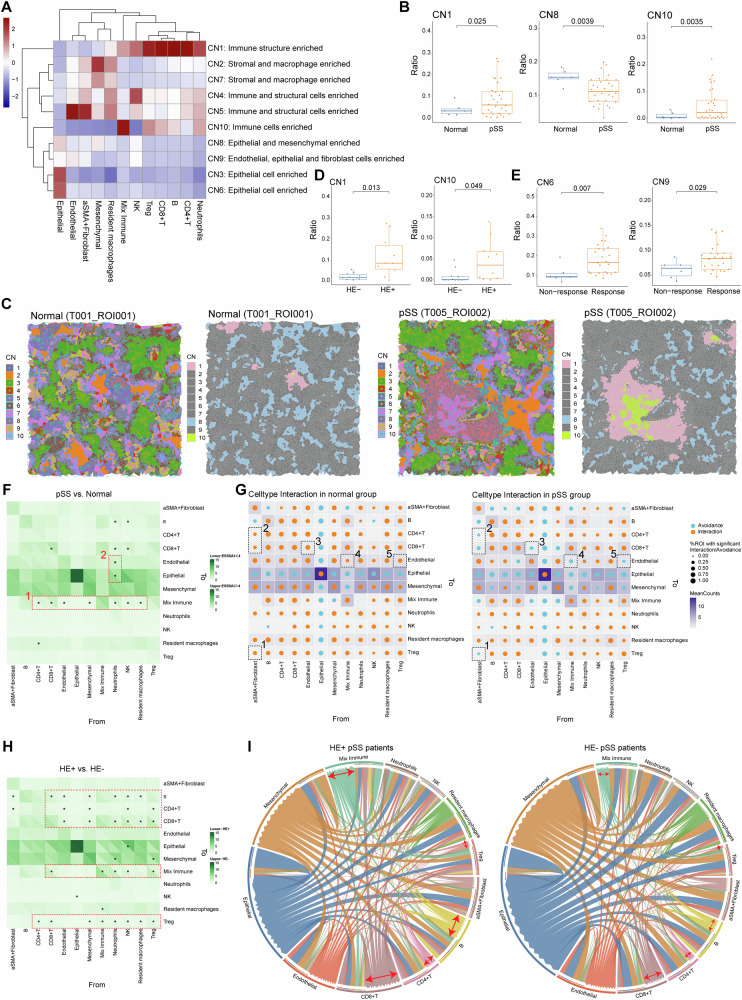
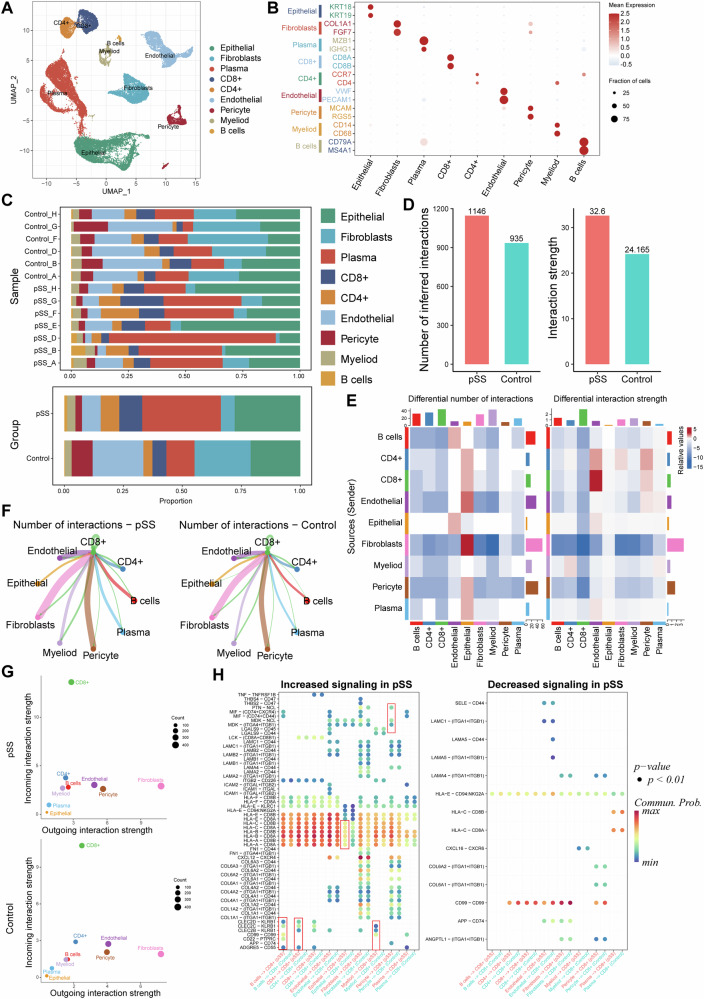
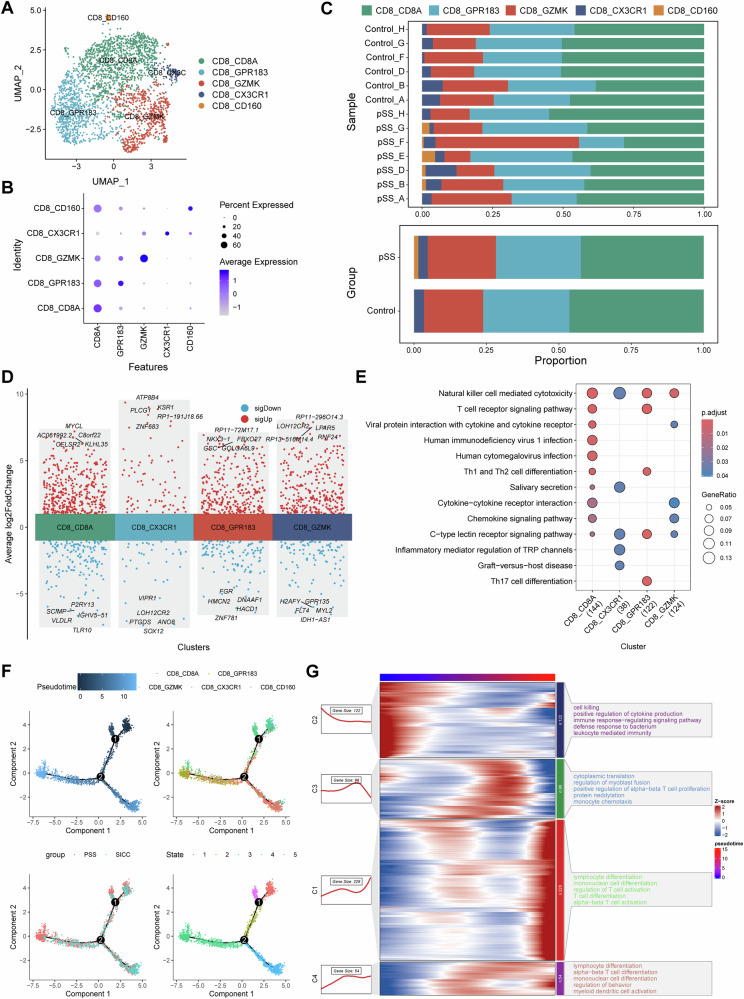
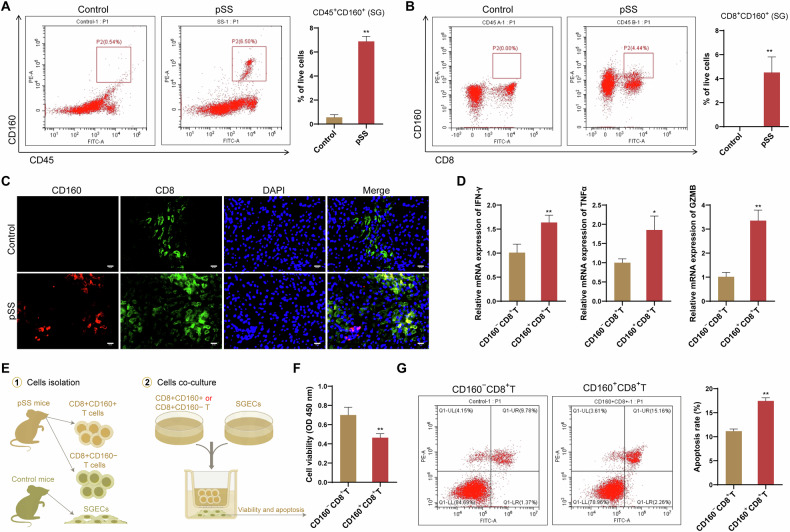
Primary Sjogren's syndrome (pSS) is a slowly progressive, systemic autoimmune disorder characterized by gradual lymphocytic infiltration of exocrine glands. However, the spatially profiling the immune microenvironment in pSS is largely unclear, limiting the understanding of the complex interplay among cells within the microenvironment. Based on imaging mass cytometry (IMC) analysis of clinical pSS samples, we first revealed that labial salivary gland (LSG) comprised of epithelial, immune cells and stromal cells, and epithelial was the main cell type in LSG. Eight immune cells populations were identified, including CD8+ T, CD4+ T, Treg, B, NK cells, neutrophils, resident macrophages and a mixed immune cell cluster. We found that CD8+ T cells, but not CD4+ T cells, were the most prominent T cells in immune infiltrates of pSS LSG. With the increase of pSS disease activity and severity, the infiltration abundance of CD8+ T cells gradually increased and was accompanied by the activation of inflammatory response. sc-RNA-seq analysis based on the GSE272409 dataset confirmed that CD8+ T cells were the main immune cells, and dominated the most intercellular ligand-receptor interactions. CD8+ T cells were further clustered into five cell subsets, of which CD160+CD8+ T cells subset appeared to present only in pSS patients. Further experiments demonstrated that CD160 expression on CD8+ T cells was associated with an enhanced expression of proinflammatory and cytotoxic cytokines IFN-γ, GZMB and TNF-α, and the injury of salivary gland epithelial cells. Besides, proportion of GZMK+CD8+ T cells subset was increased in pSS patients. Trajectory analysis confirmed an enhanced frequency of CD8+ T cell differentiation and activation during the progression of pSS. This study provided single cell profile with spatial information for analyzing the LSG immune microenvironment in pSS, which could not be achieved by conventional immunofluorescence and immunohistochemistry assays.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests. Ethical approval: For all the patients, written informed consents were obtained, and the protocol was approved by the Ethics Committee of the first affiliated hospital of Zhejiang University School of Medicine (IIT20240145B). Besides, whole animal experiments were supported by the Animal Experimental Ethics Committee of Yangzhou University (Ethics No. 202504019), which were conducted in accordance with ARRIVE guidelines.
Figures
Similar articles
-
Increased interleukin (IL)-7Rα expression in salivary glands of patients with primary Sjogren's syndrome is restricted to T cells and correlates with IL-7 expression, lymphocyte numbers and activity.Ann Rheum Dis. 2012 Jun;71(6):1027-33. doi: 10.1136/annrheumdis-2011-200744. Epub 2012 Feb 6. Ann Rheum Dis. 2012. PMID: 22312161
-
Alterations of CD8+ T cells in the blood and salivary glands of patients with primary Sjögren's syndrome.Clin Rheumatol. 2023 May;42(5):1327-1338. doi: 10.1007/s10067-022-06491-7. Epub 2023 Jan 7. Clin Rheumatol. 2023. PMID: 36609932 Free PMC article.
-
Autoantigen-specific B cells and plasma cells are prominent in areas of fatty infiltration in salivary glands of patients with primary Sjögren's syndrome.Autoimmunity. 2019 Nov-Dec;52(7-8):242-250. doi: 10.1080/08916934.2019.1684475. Epub 2019 Oct 30. Autoimmunity. 2019. PMID: 31661985
-
CD8+ T Lymphocytes: Crucial Players in Sjögren's Syndrome.Front Immunol. 2021 Jan 28;11:602823. doi: 10.3389/fimmu.2020.602823. eCollection 2020. Front Immunol. 2021. PMID: 33584670 Free PMC article. Review.
-
Salivary Gland Pathology in Sjögren's Syndrome.Rheum Dis Clin North Am. 2016 Aug;42(3):473-83. doi: 10.1016/j.rdc.2016.03.006. Epub 2016 Jun 21. Rheum Dis Clin North Am. 2016. PMID: 27431349 Review.
References
-
- Brito-Zerón P, Retamozo S, Ramos-Casals M. Sjögren syndrome. Med Clin. 2023;160:163–71. - PubMed
-
- Gran JT. Diagnosis and definition of primary Sjögren’s syndrome. Scand J Rheumatol. 2002;31:57–59. - PubMed
-
- Seror R, Nocturne G, Mariette X. Current and future therapies for primary Sjögren syndrome. Nat Rev Rheumatol. 2021;17:475–86. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
