

Developing cardiac digital twin populations powered by machine learning provides electrophysiological insights in conduction and repolarization
- PMID: 40379795
- PMCID: PMC12084159
- DOI: 10.1038/s44161-025-00650-0
Developing cardiac digital twin populations powered by machine learning provides electrophysiological insights in conduction and repolarization
Abstract
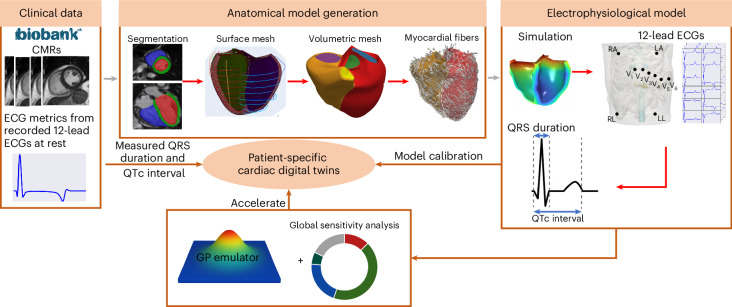
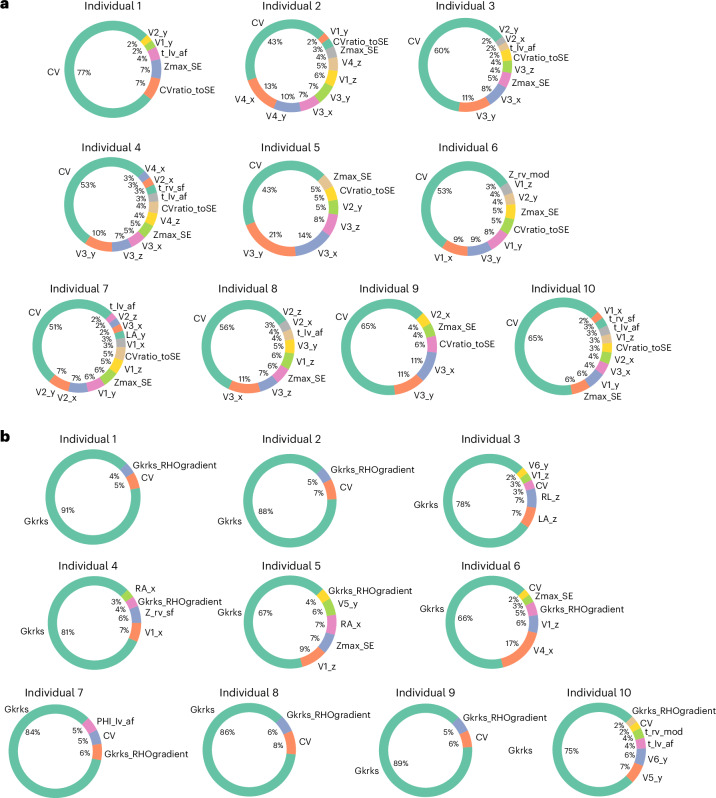
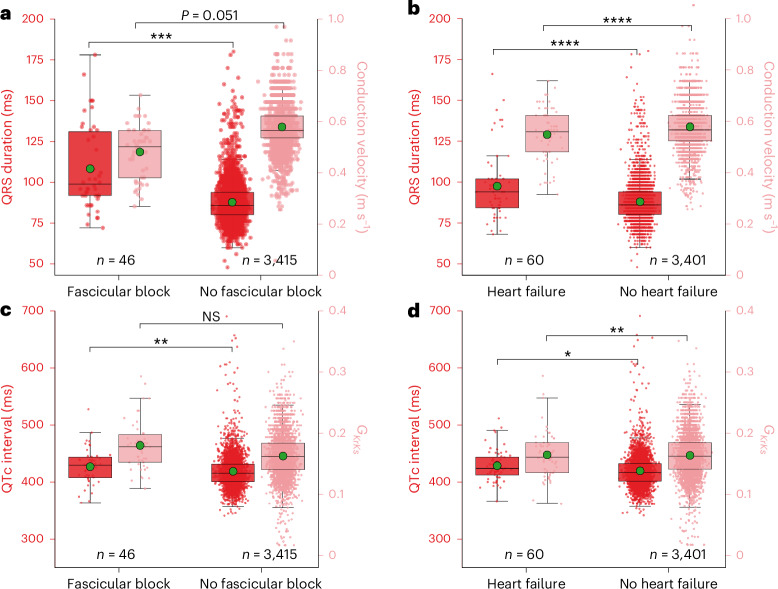
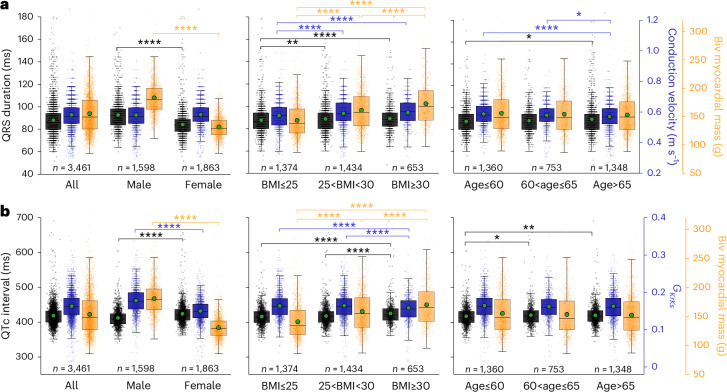
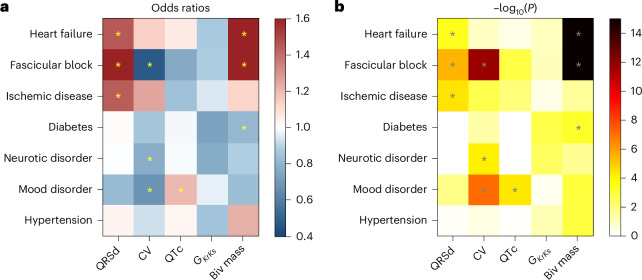
Large-cohort imaging and diagnostic studies often assess cardiac function but overlook underlying biological mechanisms. Cardiac digital twins (CDTs) are personalized physics-constrained and physiology-constrained in silico representations, uncovering multi-scale insights tied to these mechanisms. In this study, we constructed 3,461 CDTs from the UK Biobank and another 359 from an ischemic heart disease (IHD) cohort, using cardiac magnetic resonance images and electrocardiograms. We show here that sex-specific differences in QRS duration were fully explained by myocardial anatomy while their myocardial conduction velocity (CV) remains similar across sexes but changes with age and obesity, indicating myocardial tissue remodeling. Longer QTc intervals in obese females were attributed to larger delayed rectifier potassium conductance . These findings were validated in the IHD cohort. Moreover, CV and were associated with cardiac function, lifestyle and mental health phenotypes, and CV was also linked with adverse clinical outcomes. Our study demonstrates how CDT development at scale reveals biological insights across populations.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures











References
-
- Niederer, S. A., Sacks, M. S., Girolami, M. & Willcox, K. Scaling digital twins from the artisanal to the industrial. Nat. Comput. Sci.1, 313–320 (2021). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources