

Effect of chest pain center accreditation on timely reperfusion and in-hospital mortality for STEMI in China
- PMID: 40379826
- PMCID: PMC12084382
- DOI: 10.1038/s41598-025-02151-3
Effect of chest pain center accreditation on timely reperfusion and in-hospital mortality for STEMI in China
Abstract
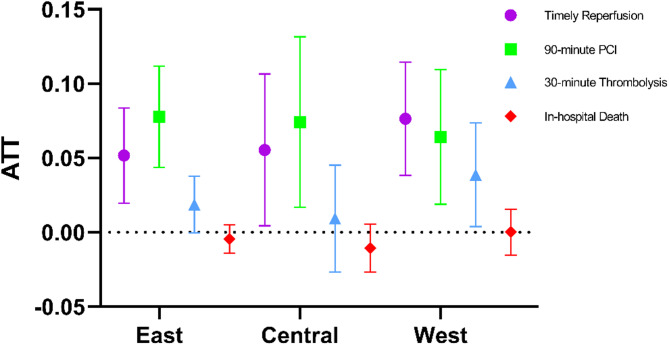
Existing studies in developing countries on the impact of chest pain center (CPC) accreditation on treatment quality have limited ability to demonstrate causal relationships. This retrospective study aims to utilize the data from national-level database and explore the impact of chest pain center certification on the treatment quality of ST-segment elevation myocardial infarction (STEMI) patients through a more appropriate method. At the hospital level, taking timely reperfusion and in-hospital mortality as outcomes, the impact was evaluated using the Counterfactual Synthetic Difference-in-Differences (CS-DID) method, a statistical technique that allows for the estimation of causal effects by comparing the differences over time between treated and non-treated groups. The results showed that CPC accreditation improved timely reperfusion of STEMI. Once a CPC was certified, without considering covariates, the timely reperfusion rate increased on average by 5.4%, the 90-min PCI rate by 7.1%, and the 30-min thrombolysis rate by 2.0% in comparison with non-accredited hospitals, and this effect shows a downward trend over time and varies between different regions. We found no evidence to confirm that CPC accreditation decreases in-hospital mortality in patients with STEMI. CPC accreditation in China has improved the timeliness of reperfusion therapy for STEMI patients. CPC accreditation and re-accreditation are crucial to maintaining high-quality care for STEMI patients.
Keywords: Accreditation; CS-DID; Chest pain center; STEMI; Timely reperfusion; Treatment quality.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Management and Outcomes of Patients With STEMI During the COVID-19 Pandemic in China.J Am Coll Cardiol. 2020 Sep 15;76(11):1318-1324. doi: 10.1016/j.jacc.2020.06.039. Epub 2020 Aug 19. J Am Coll Cardiol. 2020. PMID: 32828614 Free PMC article.
-
Regional variations in management and outcomes of patients with acute coronary syndrome in China: Evidence from the National Chest Pain Center Program.Sci Bull (Beijing). 2024 May 15;69(9):1302-1312. doi: 10.1016/j.scib.2024.03.010. Epub 2024 Mar 4. Sci Bull (Beijing). 2024. PMID: 38519397
-
Effectiveness of chest pain center accreditation on the hospital outcome of acute aortic dissection: a nationwide study in China.Mil Med Res. 2024 Aug 26;11(1):62. doi: 10.1186/s40779-024-00565-0. Mil Med Res. 2024. PMID: 39183322 Free PMC article.
-
Reperfusion strategies on the clinical outcomes of ST-elevation myocardial infarction patients over 80 years old in China.Eur Heart J Qual Care Clin Outcomes. 2025 Jan 16;11(1):28-36. doi: 10.1093/ehjqcco/qcae013. Eur Heart J Qual Care Clin Outcomes. 2025. PMID: 38337188
-
A System of Care for Patients With ST-Segment Elevation Myocardial Infarction in India: The Tamil Nadu-ST-Segment Elevation Myocardial Infarction Program.JAMA Cardiol. 2017 May 1;2(5):498-505. doi: 10.1001/jamacardio.2016.5977. JAMA Cardiol. 2017. PMID: 28273293 Free PMC article.
References
-
- Tunstall-Pedoe, H. et al. Contribution of trends in survival and coronary-event rates to changes in coronary heart disease mortality: 10-year results from 37 WHO MONICA project populations. Monitoring trends and determinants in cardiovascular disease. Lancet353 (9164), 1547–1557 (1999). - PubMed
-
- Zhou, M. et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the global burden of disease study 2013. Lancet387 (10015), 251–272 (2016). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
