

Compartmentalised mucosal and blood immunity to SARS-CoV-2 is associated with high seroprevalence before the Delta wave in Africa
- PMID: 40379979
- PMCID: PMC12084339
- DOI: 10.1038/s43856-025-00902-x
Compartmentalised mucosal and blood immunity to SARS-CoV-2 is associated with high seroprevalence before the Delta wave in Africa
Abstract
Background: The reported number of SARS-CoV-2 cases and deaths are lower in Africa compared to many high-income countries. However, in African cohorts, detailed characterisation of SARS-CoV-2 mucosal and T cell immunity are limited. We assessed the SARS-CoV-2-specific immune landscape in The Gambia during the presence of the pre-Delta variant in July 2021.
Methods: A cross-sectional assessment of SARS-CoV-2 immunity in 349 unvaccinated individuals from 52 Gambian households was performed between March-June 2021. SARS-CoV-2 spike (S) and nucleocapsid (N) specific binding antibodies were measured by ELISA, variant-specific serum neutralizing-antibodies (NAb) by viral pseudotype assays and nasal fluid IgA by mesoscale discovery assay. SARS-CoV-2 T-cell responses were evaluated using ELISpot assay.
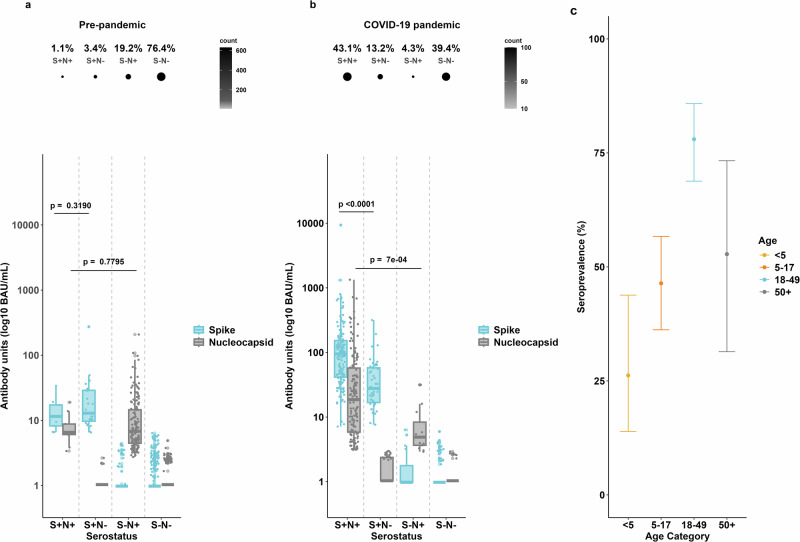
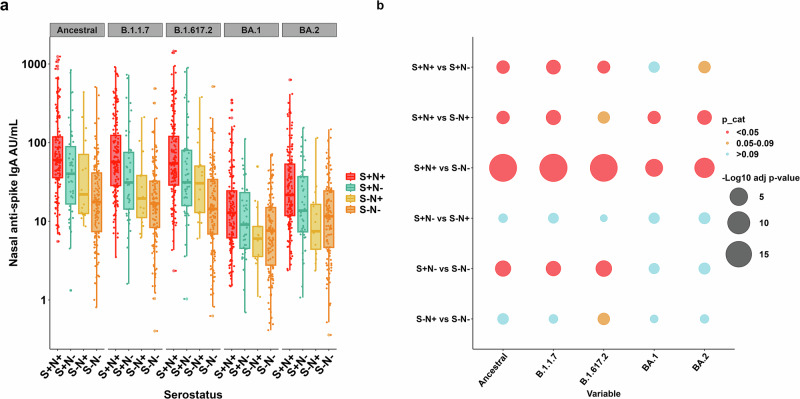
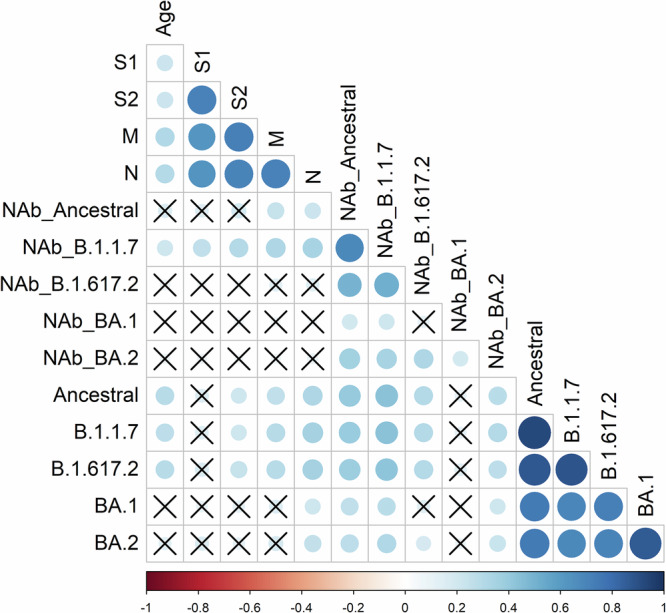
Results: We show that adjusted anti-Spike antibody seroprevalence is 56.7% (95% confidence interval (CI) 49.0-64.0), with lower rates in children <5 years (26.2%, 13.9-43.8) and 5-17 years (46.4%, 36.2-56.7) compared to adults 18-49 years (78.4%, 68.8-85.8). Among spike-seropositive individuals, NAb titres are highest against Alpha variant (median IC50 110), with 27% showing pre-existing Delta variant titres >1:50. T-cell responses are higher in spike-seropositive individuals, although 34% of spike-seronegative individuals show responses to at least one antigen pool. We observe strong correlations within SARS-CoV-2 T-cell, mucosal IgA, and serum NAb responses.
Conclusions: High SARS-CoV-2 seroprevalence in The-Gambia induce mucosal and blood immunity, reducing Delta and Omicron impact. Children are relatively protected from infection. T-cell responses in seronegative individuals may indicate either pre-pandemic cross-reactivity or individuals with a T-cell dominated response to SARS-CoV-2 infection with absent or poor humoral responses.
Plain language summary
The COVID-19 pandemic caused many illnesses and deaths worldwide. In Africa, the reported number of COVID-19 cases remained low and while under-reporting may have played a role, no increase in deaths was seen in The Gambia during the first year of the COVID-19 pandemic. There is limited data on how the immune system of Africans respond to COVID-19 infections. Our aim was to assess COVID-19 immune responses using blood and nasal swabs collected from the participants. Measurement of immune cell function and antibody levels, showed that COVID-19 infection activated different specialized cells of the immune system, including certain white blood cells (T cells) and antibodies. Antibodies are proteins made by the cells in our body, found in the blood and mucous membranes and protect against infection. We also found that COVID-19 infection rates were higher in adults compared to children and that the immune responses from an infection with earlier COVID-19 variants may have conferred protection against infection with later variants. These findings contribute to our understanding of how Africans of different ages responded to COVID-19 infection.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures


References
-
- World Health Organization. Data at WHO. https://data.who.int/dashboards/covid19/cases (2024).
-
- World Health Organization. COVID-19 response in the Gambia—documenting WHO’s support in the COVID19 response. 1–44 (2024).
LinkOut - more resources
Full Text Sources
Miscellaneous
