

A plasma 9-microRNA signature for lung cancer early detection: a multicenter analysis
- PMID: 40380218
- PMCID: PMC12085043
- DOI: 10.1186/s40364-025-00787-x
A plasma 9-microRNA signature for lung cancer early detection: a multicenter analysis
Abstract
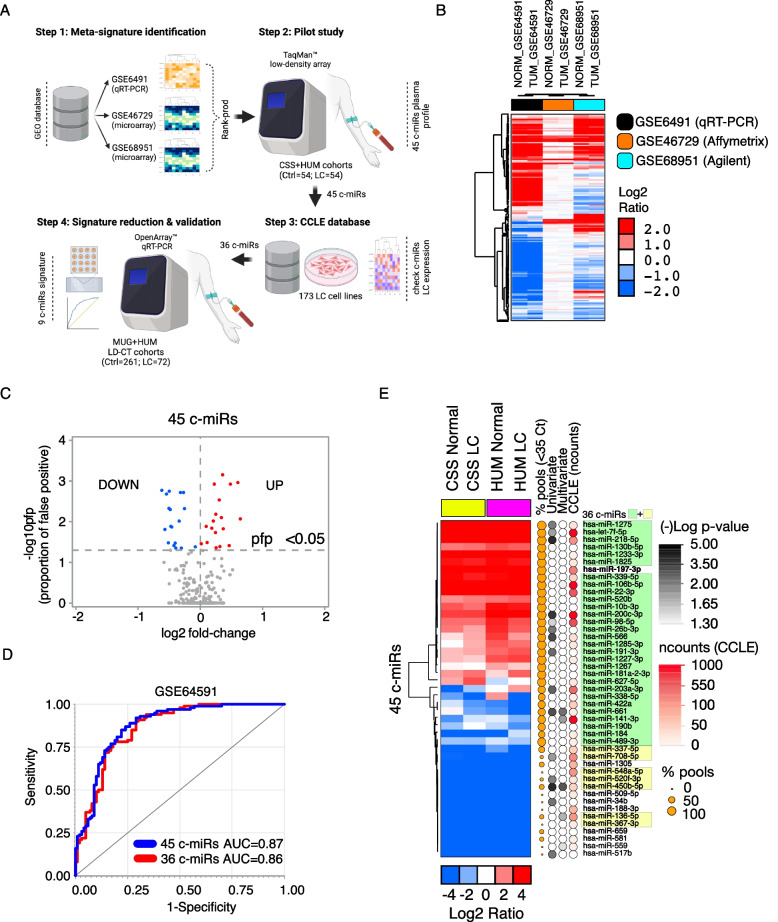
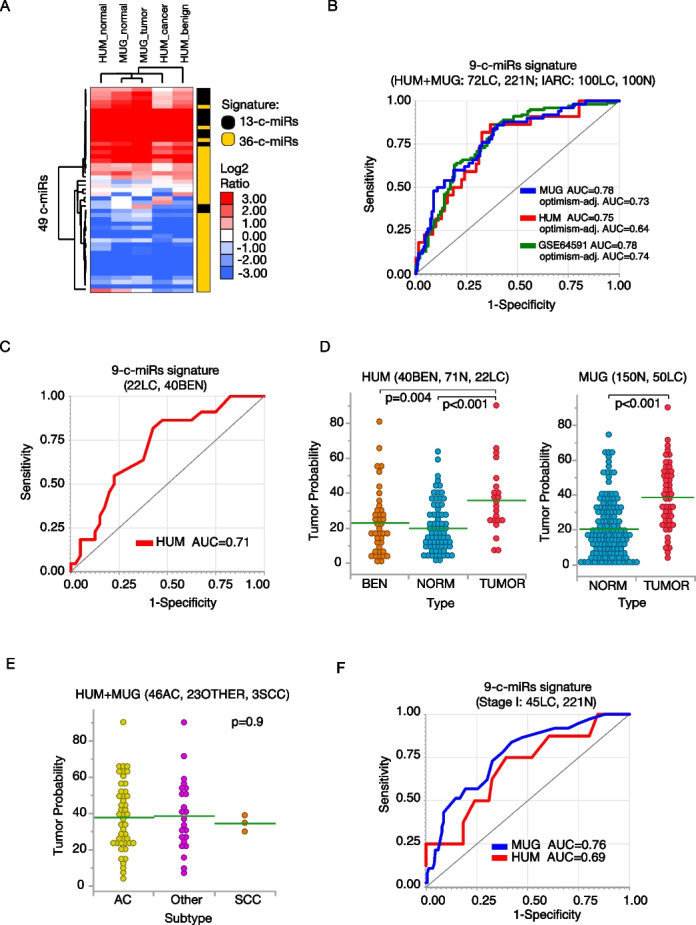
Lung cancer remains the leading cause of cancer-related deaths worldwide. Low-dose computed tomography (LD-CT) screening, combined with effective minimally invasive molecular testing such circulating microRNA, has the potential to reduce the burden of lung cancer. However, their clinical application requires further validation, including studies across diverse patient cohorts from different countries. In this study, we propose a signature of 9 circulating miRNAs derived from a robust multi-platform workflow with a multi-center design, for a total of 276 lung cancer and 451 non-cancer controls, based on the data from two European LD-CT screening cohorts (Poland and Italy). The classification performance of the signature was stable in the two screening cohorts, with AUC=0.78 (SE, 76%; SP, 67%; ACC=70%), and AUC=0.75 (SE, 82%; SP, 68%; ACC=71%) in the Polish and Italian cohorts, respectively. The diagnostic accuracy of the signature was remarkably independent of age, gender, smoking (status and intensity), nodule size, and density. Additionally, the signature demonstrated strong performance in detecting stage I lung cancer, with AUC=0.76 (95%CI: 0.68-0.84), and 0.69 (95%CI: 0.49-0.89) in the Polish and Italian cohorts respectively, with a prediction ability of 63-73%. The signature's ability to discriminate benign nodules was satisfactory, with AUC=0.71 (95%CI: 0.58-0.84). The proposed panel of 9 circulating miRNAs provides a robust and precise diagnostic tool to substantially advance the effectiveness of the LD-CT screening program.
Keywords: Early diagnosis; Liquid biopsy; Lung cancer; Machine learning; MicroRNA.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Institutional Review Board (Medical University of Gdansk approval numbers NKEBN/42/2009 and NKBBN/376/2014; and Humanitas Clinical and Research Center approval number CE Humanitas ex DM 390/18; Fondazione IRCCS Casa Sollievo della Sofferenza approval number BIO-POLMONE - V1.0_08 Giu 16) approved this study, and informed consent was obtained from all the participants. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clinicians. 2024;74:229–63. - PubMed
-
- De Koning HJ, Van Der Aalst CM, De Jong PA, Scholten ET, Nackaerts K, Heuvelmans MA, et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N Engl J Med. 2020;382:503–13. - PubMed
-
- Jonas DE, Reuland DS, Reddy SM, Nagle M, Clark SD, Weber RP, et al. Screening for lung cancer with low-dose computed tomography: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2021;325:971. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
