

Individualized mean arterial pressure targets in critically ill patients guided by non-invasive cerebral-autoregulation: a scoping review
- PMID: 40380314
- PMCID: PMC12084981
- DOI: 10.1186/s13054-025-05432-5
Individualized mean arterial pressure targets in critically ill patients guided by non-invasive cerebral-autoregulation: a scoping review
Abstract
Background: Current guidelines recommend a uniform mean arterial pressure (MAP) target for resuscitating critically ill patients; for example, 65 mmHg for patients with sepsis and post-cardiac arrest. However, since cerebral autoregulation capacity likely varies widely in patients, uniform target may be insufficient in maintaining cerebral perfusion. Personalized MAP targets, based on a non-invasive determination of cerebral autoregulation, may optimize perfusion and reduce complications.
Objectives: This scoping review summarizes the numerical values, feasibility, and clinical data on personalized MAP targets in critically ill patients. The focus is on non-invasive monitoring, such as near-infrared spectroscopy and transcranial doppler ultrasound, due to their safety, practicality and applicability to patients with- and without brain injury.
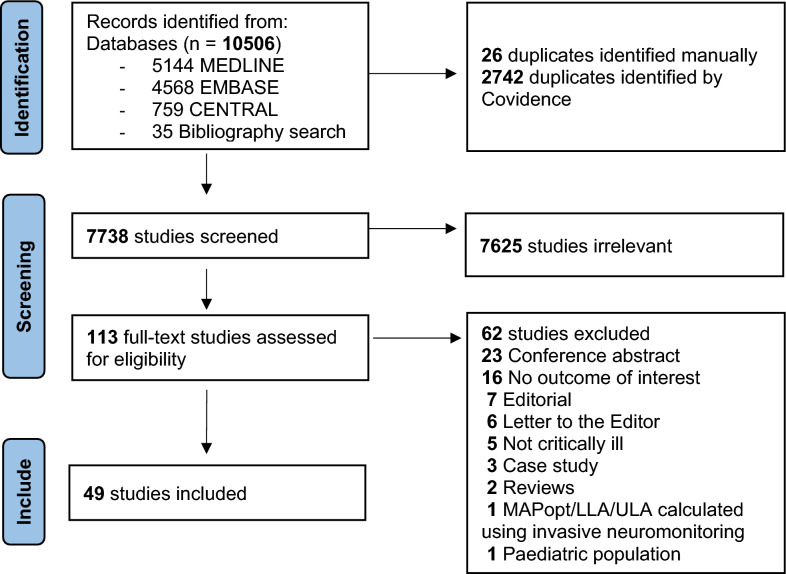
Methods: Following PRISMA-ScR guidelines, a systematic search of Ovid MedLine, Embase (Ovid), and the Cochrane Library (Wiley) was conducted on September 28, 2023. Two independent reviewers screened titles, abstracts, and full texts for eligibility and manually reviewed references.
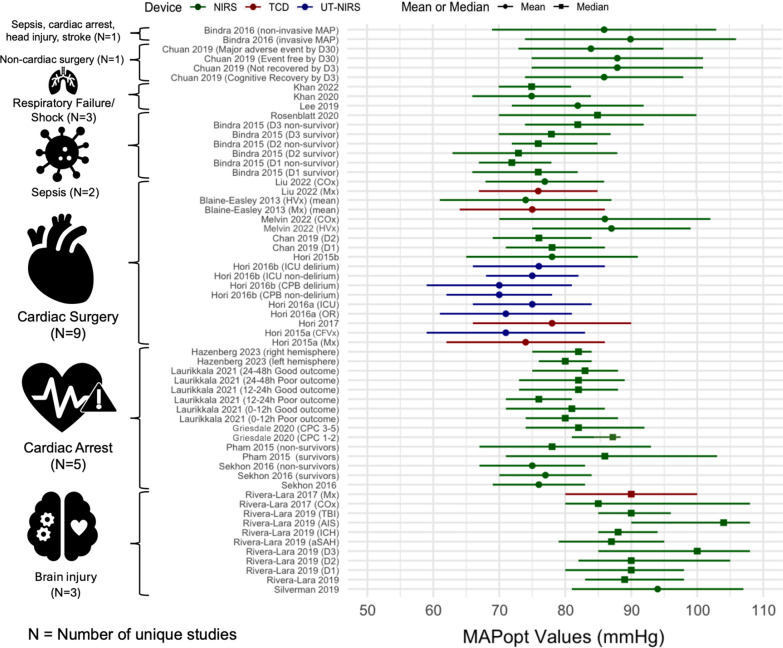
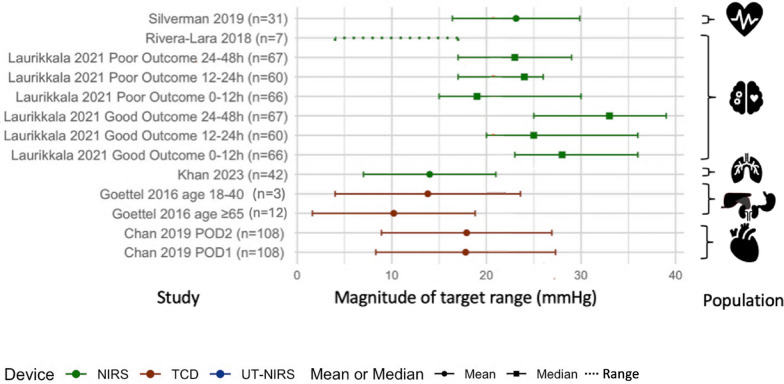
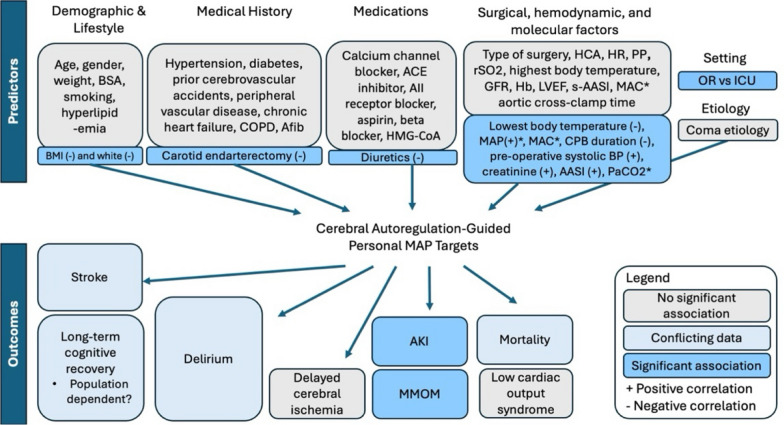
Results: Of 7,738 studies were identified, 49 met the inclusion criteria. Of these, 45 (92%) were observational and 4 (8%) were interventional. Patient populations included cardiac surgery (26, 53%), non-cardiac major surgery (4, 8%), cardiac arrest (8, 16%), brain injury (7, 14%), respiratory failure and shock (3, 6%), and sepsis (3, 6%). Optimal MAP was reported in 24 (49%), lower limit of autoregulation in 23 (47%), and upper limit of autoregulation in 10 studies (20%). Thirty-four studies reported partial data loss due to software failures, anomalous data, insufficient natural MAP fluctuation, and workflow barriers. Available randomized controlled trials (RCT) identified challenges with maintaining patients within their target range. Studies explored the associations between personalized MAP targets and a wide range of neurological and non-neurological outcomes, with the most significant and consistent associations identified for acute kidney injury and major morbidity and mortality. Ten studies investigated demographic predictors identifying only few predictors of personalized targets.
Conclusion: Preliminary investigations suggest considerable variability in personalized MAP targets, which may explain differences in clinical outcomes among critically ill populations. Key gaps remain, including a lack of observational studies in critically ill subpopulations other than cardiac surgery and well-designed RCTs. Resolving identified feasibility barriers might be crucial to successfully carrying out future studies.
Keywords: Arterial pressure; Autoregulation; Big data; Cerebral vascular circulation; Near-infrared spectroscopy; Precision medicine; Transcranial Doppler ultrasonography.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
