

Predictors of difficulty in robotic splenic flexure mobilization during rectal cancer surgery
- PMID: 40381041
- PMCID: PMC12085353
- DOI: 10.1007/s00384-025-04916-8
Predictors of difficulty in robotic splenic flexure mobilization during rectal cancer surgery
Abstract
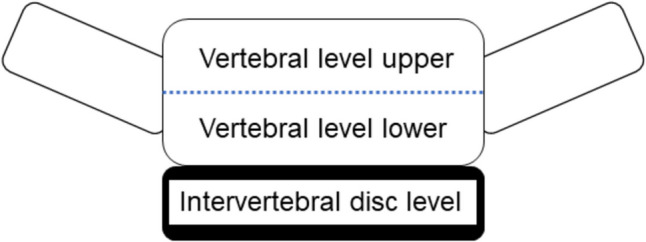
Purpose: In surgery for rectal cancer, splenic flexure mobilization is sometimes necessary to ensure a tension-free colorectal anastomosis with adequate blood supply. Splenic flexure mobilization is regarded as a challenging and risky maneuver, but there are no clear indicators of its difficulty in rectal cancer surgery. This study evaluated the impact of clinical and anatomical factors, including splenic flexure height measured qualitatively on the basis of vertebral level using computed tomography, on the difficulty of splenic flexure mobilization during rectal cancer surgery.
Methods: The enrolled patients underwent robotic splenic flexure mobilization during rectal surgery for primary rectal cancer at Shizuoka Cancer Center in Japan between December 2011 and March 2022. All patients were scheduled to undergo splenic flexure mobilization preoperatively, and all procedures were carried out following a standardized approach. Linear regression analysis was conducted to determine the clinical and anatomical factors significantly influencing the operative time of the abdominal phase, which is defined as the duration from lymph node dissection around the inferior mesenteric artery to the mobilization of the sigmoid and descending colon, including the splenic flexure.
Results: The median operative time for the abdominal phase was 88 min (range, 39-179 min). Univariate analysis revealed that the following variables were significantly correlated with a prolonged abdominal phase: higher body mass index, larger visceral fat area, and higher splenic flexure. In a multiple linear regression analysis, only higher splenic flexure remained significantly associated with a longer abdominal phase (p < 0.01).
Conclusions: Splenic flexure height measured on the basis of vertebral level using computed tomography may be useful for predicting the difficulty of robotic splenic flexure mobilization in surgery for rectal cancer.
Keywords: Operative time; Robotic surgery; Splenic flexure mobilization; Surgical difficulty.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This study was approved by the Institutional Review Board of Shizuoka Cancer Center Hospital (institutional code J2022-58–2022-1–3). Competing interests: The authors declare no competing interests.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
