

Comparative efficacy of subthreshold micropulse laser versus conventional laser therapy in central serous chorioretinopathy
- PMID: 40381063
- PMCID: PMC12085379
- DOI: 10.1007/s10103-025-04473-0
Comparative efficacy of subthreshold micropulse laser versus conventional laser therapy in central serous chorioretinopathy
Abstract
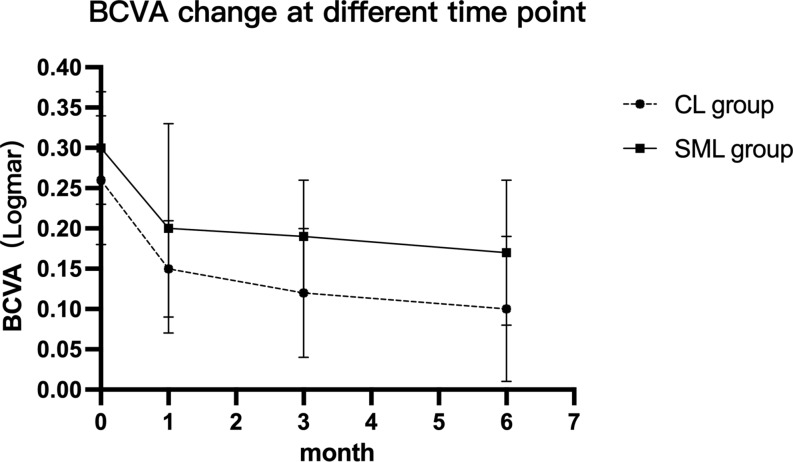
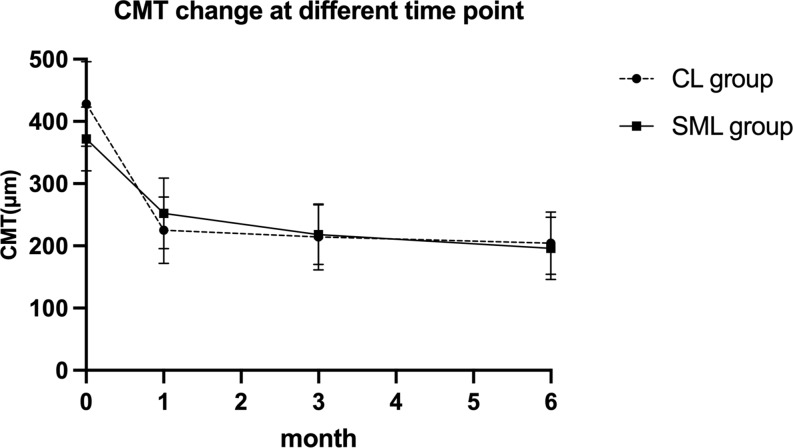
Subthreshold micropulse laser (SML) and conventional laser photocoagulation (CLP) have established efficacy in treating central serous chorioretinopathy (CSC), but systematic comparisons of their effectiveness, safety, and long-term outcomes remain lacking.We carried out this retrospective study. A total of 109 eyes from 109 CSC patients were included, with 53 eyes in the conventional laser group and 56 eyes in the SML group. The SML group was treated with a 577-nm wavelength laser, targeting areas of leakage and subretinal fluid (SRF). For patients without identifiable leakage points, the treatment area covered the SRF region. The conventional laser group received single-spot laser treatment with a laser spot reaction of ≤ grade 1, targeting leakage points identified by early-phase fluorescein angiography (FFA). Disease duration, leakage points on FFA, best-corrected visual acuity (BCVA) during follow-up, central macular thickness (CMT), SRF resolution, and safety were analyzed. The mean follow-up duration was 6.90 ± 2.77 months. The conventional laser group had a shorter mean disease duration compared to the SML group (P = 0.002), and there was a significant difference in the distribution of leakage points between the two groups (P = 0.000). At 6 months post-treatment, compared to baseline, the BCVA change was 0.24 ± 0.28 in the CL group (P = 0.02) and 0.19 ± 0.18 in the SML group (P = 0.04). There were no significant differences in BCVA between the two groups at any follow-up time point, though. CMT changes from baseline to final follow-up demonstrated a mean reduction of 228.00 ± 181.01 μm in the CL group versus 176.97 ± 143.39 μm in the SML group (both P < 0.001). No significant differences were observed in mean CMT or final OCT changes between the two groups at any follow-up time point. The complete SRF resolution rates were 83.01% in the conventional laser group and 87.50% in the SML group (P = 0.59).Both SML and CL treatments are safe and effective for CSC. CL therapy is a safe and effective option for patients with acute disease, clearly identifiable leakage points located > 250 μm from the foveal center, while SML is preferable for patients with longer disease duration, unclear leakage points, or leakage points located within 250 μm of the foveal center. Clinical trial number: Not applicable.
Keywords: Central serous chorioretinopathy; Conventional laser; Subthreshold micropulse laser.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: All patients provided written informed consent to participate in accordance with the Helsinki Declaration guidelines. Informed consents have been obtained to publish the images in an online open-access publication. The Medical Ethics Committee of Peking University People’s Hospital approved this study (2016PHA008). All methods were carried out in accordance with relevant guidelines and regulations of retinal vein occlusion. All experimental protocols were approved by Committee of Clinical Drug Trials, Peking University People’s Hospital. Informed consent was obtained from all patients and/or their legal guardian(s). Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Comparative efficacy of subthreshold micropulse laser therapy for chronic central serous chorioretinopathy: Navigated vs. non-navigated approach.J Fr Ophtalmol. 2025 May;48(5):104483. doi: 10.1016/j.jfo.2025.104483. Epub 2025 Mar 13. J Fr Ophtalmol. 2025. PMID: 40086045
-
Subthreshold 577 nm micropulse laser treatment for central serous chorioretinopathy.PLoS One. 2017 Aug 29;12(8):e0184112. doi: 10.1371/journal.pone.0184112. eCollection 2017. PLoS One. 2017. PMID: 28850595 Free PMC article.
-
Efficacy of subthreshold micropulse laser for chronic central serous chorioretinopathy: A meta-analysis.Photodiagnosis Photodyn Ther. 2022 Sep;39:102931. doi: 10.1016/j.pdpdt.2022.102931. Epub 2022 May 27. Photodiagnosis Photodyn Ther. 2022. PMID: 35636735
-
Comparison of subthreshold micropulse laser (577 nm) treatment and half-dose photodynamic therapy in patients with chronic central serous chorioretinopathy.Eye (Lond). 2016 Oct;30(10):1371-1377. doi: 10.1038/eye.2016.142. Epub 2016 Jul 8. Eye (Lond). 2016. PMID: 27391938 Free PMC article.
-
Monotherapy laser photocoagulation for diabetic macular oedema.Cochrane Database Syst Rev. 2018 Oct 15;10(10):CD010859. doi: 10.1002/14651858.CD010859.pub2. Cochrane Database Syst Rev. 2018. PMID: 30320466 Free PMC article.
References
-
- Feenstra HMA, van Dijk EHC, Cheung CMG, Ohno-Matsui K, Lai TYY, Koizumi H, Larsen M, Querques G, Downes SM, Yzer S et al (2024) Central serous chorioretinopathy: an evidence-based treatment guideline. Prog Retin Eye Res 101:101236. 10.1016/j.preteyeres.2024.101236 - PubMed
-
- Kitzmann AS, Pulido JS, Diehl NN, Hodge DO, Burke JP (2008) The incidence of central serous chorioretinopathy in olmsted County, Minnesota, 1980–2002. Ophthalmology 115:169–173. 10.1016/j.ophtha.2007.02.032 - PubMed
-
- van Rijssen TJ, van Dijk EHC, Yzer S, Ohno-Matsui K, Keunen JEE, Schlingemann RO, Sivaprasad S, Querques G, Downes SM, Fauser S et al (2019) Central serous chorioretinopathy: towards an evidence-based treatment guideline. Prog Retin Eye Res 73:100770. 10.1016/j.preteyeres.2019.07.003 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
