

Circadian rhythm disruption by PARP inhibitors correlates with treatment toxicity in patients with ovarian cancer and is a predictor of side effects
- PMID: 40382284
- PMCID: PMC12173083
- DOI: 10.1016/j.ebiom.2025.105764
Circadian rhythm disruption by PARP inhibitors correlates with treatment toxicity in patients with ovarian cancer and is a predictor of side effects
Abstract
Background: Ovarian cancer is among the most lethal malignancies in women. The advent of PARP inhibitors (PARPi) has improved outcomes. However, treatment-related toxicity remains a critical challenge, impacting patient quality of life and treatment adherence.
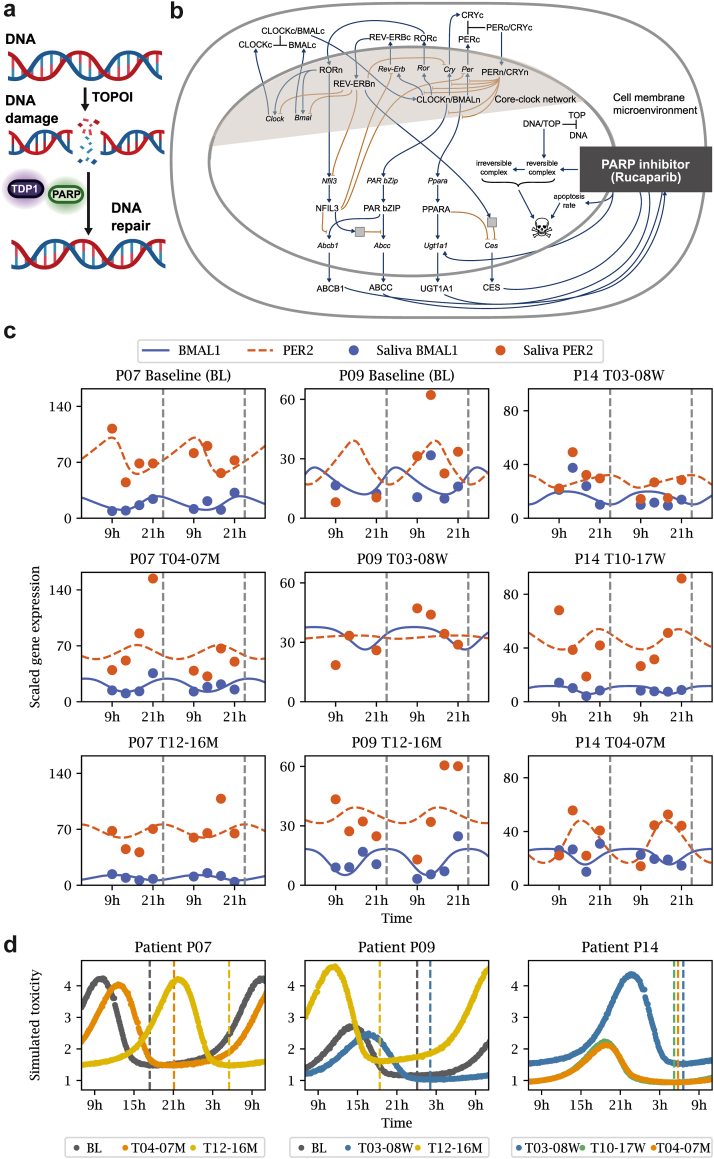
Methods: In a circadian sub-study of the MAMOC trial-a double-blind, phase III study-42 patients (FIGO stage IIIA-IV) were randomised in a 2:1 ratio to receive rucaparib or placebo. In a subset of these patients, we performed differential gene expression and rhythmicity analysis on up to 800 genes, including clock and clock-controlled genes. Machine learning algorithms and mathematical modelling were employed to simulate patient-specific toxicity profiles and to explore correlations between gene expression patterns and treatment-related side effects.
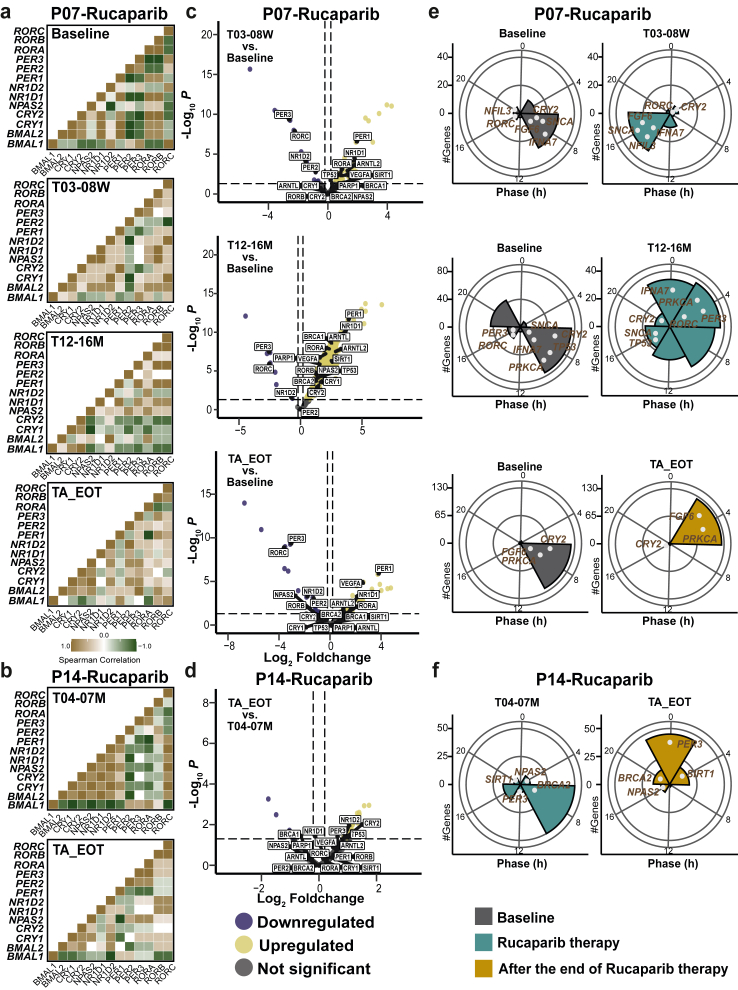
Findings: Our analysis revealed significant disruptions in circadian rhythms, specifically in the expression of the core clock genes BMAL1 and PER2, following treatment. These disruptions strongly correlated with the severity and frequency of side effects, including nausea and fatigue, displaying opposite trends between the placebo and rucaparib-treated groups. K-means clustering successfully distinguished rucaparib-treated patients from those receiving placebo based on BMAL1 phase and gene expression profiles. In addition, rucaparib therapy also altered the expression of several clock-controlled genes, including SIRT1, BRCA1, BRCA2, and TP53. Notably, our data suggest that individual differences in circadian rhythms may lead to distinct 24-h toxicity profiles among patients.
Interpretation: These findings suggest that circadian rhythm dysregulation may contribute to the toxicity of PARPi therapy. Aligning treatment timing with circadian rhythms could mitigate these adverse effects, and improve patient outcomes.
Funding: This study was funded by the Dr. Rolf Schwiete Stiftung and the MSH Medical School Hamburg, Germany. The MAMOC trial (ClinicalTrials.gov: NCT04227522) was funded by Clovis Oncology, United States.
Keywords: Adverse events; Chronotherapy; Circadian profiles; Circadian rhythms; Mathematical modelling; Ovarian cancer; PARP inhibitors; Rucaparib.
Copyright © 2025 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests The work in the group of A.R. relative to this manuscript has been financed by the MSH Medical School Hamburg, the Digital Health Accelerator Program of the Charité/BIH Berlin Institute of Health, and by the Dr. Rolf Schwiete Stiftung. A.R. is CEO of TimeTeller GmbH and has granted and pending patents regarding the characterisation of circadian rhythms in saliva for different applications. J.H. is currently at the Leibniz Institute for Resilience Research, Mainz and funded by the Boehringer Ingelheim Foundation. B.C. received honoraria from AstraZeneca and MSD. R.W. received honoraria for lectures by AstraZeneca and GSK, and received travel support from GSK for attending the ESMO conference in 2022. J.S has received funding from Roche Pharma, AstraZeneca, Bayer, Clovis Oncology, GSK, Lilly, Tesaro, and MSD for the MAMOC study; has received consulting fees from Tesaro, Merck, Pfizer, PharmaMar, Clovis Oncology, AstraZeneca, Roche Pharma, GlaxoSmith, MSD, Eisai, Novocure, Oncoinvent, Esai, Tubulis, Immunogen, AbbVie, GSK, Bayer, Vifor Pharma, Hexal AG, Novartis Pharma; has received honoraria from Tesaro, Merck, Pfizer, PharmaMar, Clovis Oncology, AstraZeneca, Roche Pharma; GlaxoSmith, MSD, Eisai, Novocure, Oncoinvent, Esai, Tubulis, Immunogen, AbbVie, GSK, Bayer, Vifor Pharma, Hexal AG, Novartis Pharma; has served a leadership role at NOGGO, AGO, ENGAGe, ENGOT, Deutsche Stiftung für Eierstockkrebs. E.I.B received funding from Clovis Oncology for the MAMOC study; has received honoraria from AstraZeneca, Abbvie, Immunogen, GSK; has received travel support from AstraZeneca; has participated on an Advisory Board for TORL-bio, Tubulis, MSD, GSK, PharmaEnd, Myriad, Immunogen; and is a medical director of the NOGGO. All other authors declare no competing interests.
Figures







References
-
- Webb P.M., Jordan S.J. Global epidemiology of epithelial ovarian cancer. Nat Rev Clin Oncol. 2024;21(5):389–400. - PubMed
-
- Pujade-Lauraine E., Selle F., Scambia G., et al. Maintenance olaparib rechallenge in patients with platinum-sensitive relapsed ovarian cancer previously treated with a PARP inhibitor (OReO/ENGOT-ov38): a phase IIIb trial. Ann Oncol. 2023;34(12):1152–1164. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
