

Neutrophil to high-density lipoprotein cholesterol ratio as a potential inflammatory marker for predicting all-cause mortality in out-of-hospital cardiac arrest survivors
- PMID: 40382458
- PMCID: PMC12085707
- DOI: 10.1038/s41598-025-01951-x
Neutrophil to high-density lipoprotein cholesterol ratio as a potential inflammatory marker for predicting all-cause mortality in out-of-hospital cardiac arrest survivors
Abstract
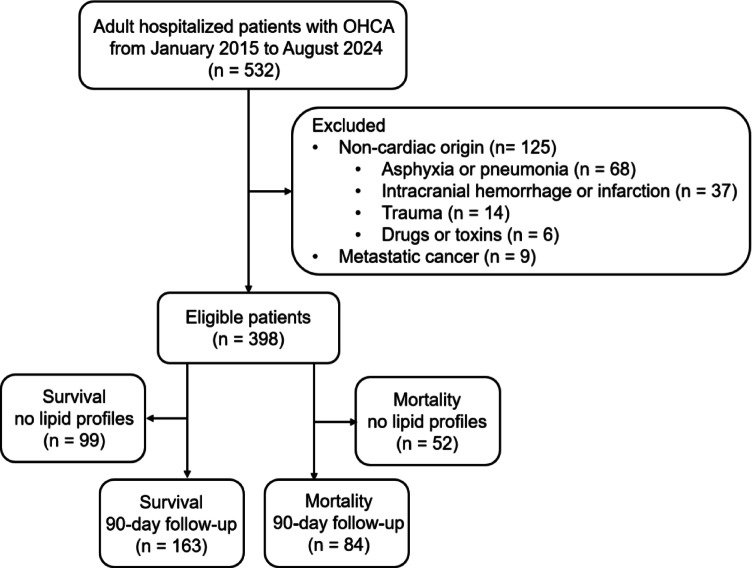
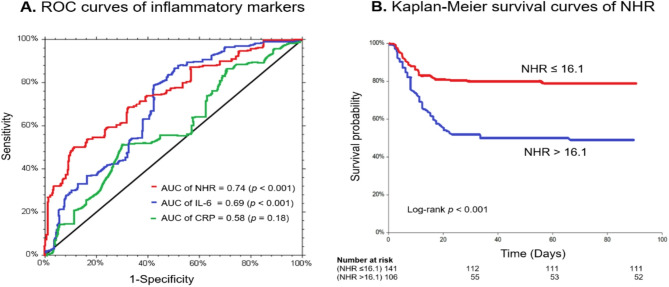
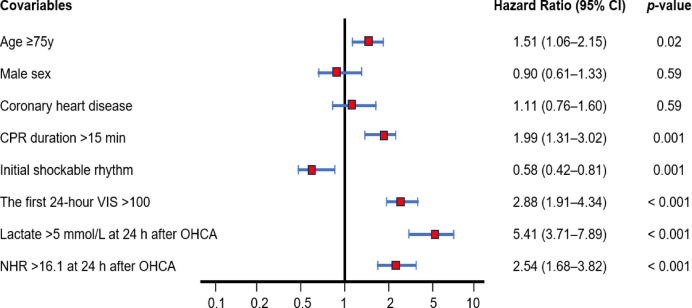
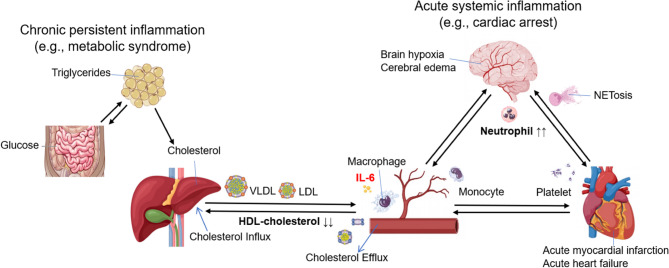
Out-of-hospital cardiac arrest (OHCA) survivors have more than one-third mortality rate. Numerous inflammatory indicators are available, and it should be feasible to identify a fast and accurate way to aid medical decisions. This retrospective cohort study included 247 patients with OHCA, hospitalized between January 2015 and August 2024. The study was conducted in the intensive care unit of China Medical University Hospital, Taichung, Taiwan. A variety of inflammatory markers, including interleukin-6, neutrophil to high-density lipoprotein cholesterol ratio (NHR), and C-reactive protein, were screened at 24 h after OHCA. The primary endpoint was the 90-day all-cause mortality. Receiver operating characteristic (ROC) curves and Kaplan-Meier survival curves of NHR were analyzed. Possible risk factors for all-cause mortality were estimated by Cox regression modeling. NHR and interleukin-6 were similarly predictive of all-cause mortality in inflammatory response, and both were superior to C-reactive protein at 24 h after OHCA (p < 0.001). The area under the ROC curve of NHR was 0.74 (95% confidence interval [CI]: 0.66-0.81, p < 0.001), sensitivity: 0.68, and specificity: 0.68, and NHR = 16.1. The 90-day all-cause mortality rate for NHR > 16.1 compared to those with NHR ≤ 16.1 was 0.51 and 0.21, respectively, according to Kaplan-Meier curves analysis. The hazard ratio for NHR > 16.1 was 2.54 (95% CI: 1.68-3.82, p < 0.001). An NHR > 16.1 at 24 h after OHCA is a potential inflammatory marker for predicting all-cause mortality.
Keywords: Cardiac arrest; High-density lipoprotein cholesterol; Neurological outcomes; Neutrophils; Systemic inflammatory response.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: The study was approved by the institutional review board of the China Medical University Hospital (CMUH104-REC3-058 and CMUH112-REC3-016) for data collection and analysis. Informed consent: Verbal and written informed consent have been obtained from all participant proxies.
Figures
Similar articles
-
Neutrophil to high-density lipoprotein ratio has a superior prognostic value in elderly patients with acute myocardial infarction: a comparison study.Lipids Health Dis. 2020 Apr 4;19(1):59. doi: 10.1186/s12944-020-01238-2. Lipids Health Dis. 2020. PMID: 32247314 Free PMC article.
-
Prognostic Value of Leucocyte to High-Density Lipoprotein-Cholesterol Ratios in COVID-19 Patients and the Diabetes Subgroup.Front Endocrinol (Lausanne). 2021 Sep 13;12:727419. doi: 10.3389/fendo.2021.727419. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34589058 Free PMC article.
-
Combined impact of neutrophil-to-high-density lipoprotein cholesterol ratio (NHR) and cognitive function on all-cause mortality in older adults: a population-based study.Lipids Health Dis. 2025 Mar 6;24(1):83. doi: 10.1186/s12944-025-02501-0. Lipids Health Dis. 2025. PMID: 40050983 Free PMC article.
-
Neutrophils to high-density lipoprotein cholesterol ratio as a new prognostic marker in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: a retrospective study.BMC Cardiovasc Disord. 2022 Oct 5;22(1):434. doi: 10.1186/s12872-022-02870-9. BMC Cardiovasc Disord. 2022. PMID: 36199038 Free PMC article.
-
Inflammatory response after out-of-hospital cardiac arrest-Impact on outcome and organ failure development.Acta Anaesthesiol Scand. 2023 Oct;67(9):1273-1287. doi: 10.1111/aas.14291. Epub 2023 Jun 20. Acta Anaesthesiol Scand. 2023. PMID: 37337696 Review.
References
-
- Geri, G. et al. Etiological diagnoses of out-of-hospital cardiac arrest survivors admitted to the intensive care unit: insights from a French registry. Resuscitation117, 66–72. 10.1016/j.resuscitation.2017.06.006 (2017). - PubMed
-
- Chong, J. Y. et al. Interleukin-6 as a potential predictor of neurologic outcomes in cardiac arrest survivors who underwent target temperature management. J. Emerg. Med.59, 828–835. 10.1016/j.jemermed.2020.09.021 (2020). - PubMed
-
- Seppä, A. M. J., Skrifvars, M. B. & Pekkarinen, P. T. Inflammatory response after out-of-hospital cardiac arrest-Impact on outcome and organ failure development. Acta Anaesthesiol. Scand.67, 1273–1287. 10.1111/aas.14291 (2023). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
