

Spatiotemporal effects of urban micro-scale built environment on cardiovascular diseases
- PMID: 40382476
- PMCID: PMC12085694
- DOI: 10.1038/s41598-025-02603-w
Spatiotemporal effects of urban micro-scale built environment on cardiovascular diseases
Abstract
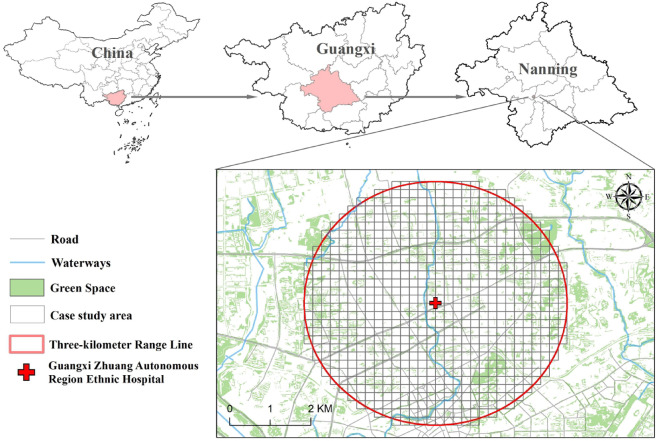
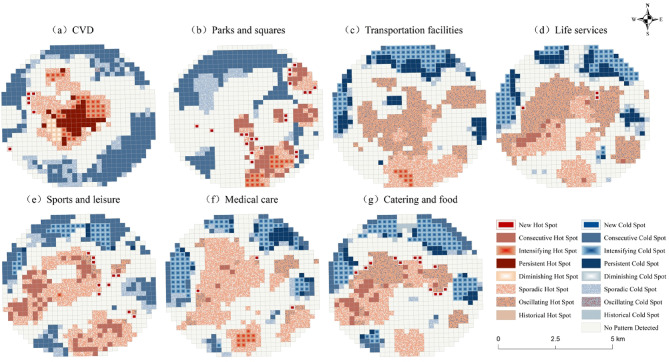
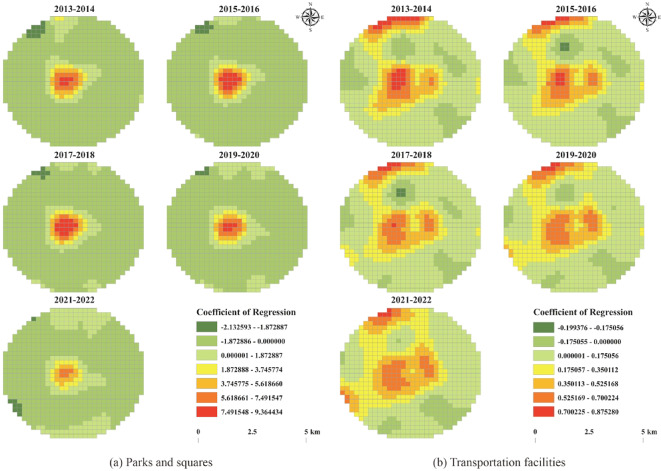
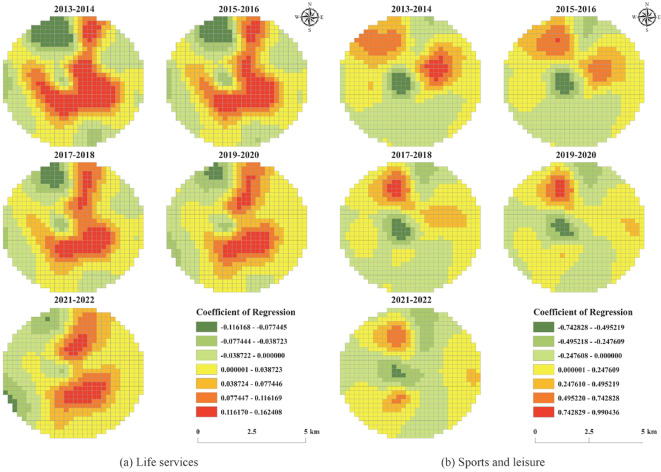
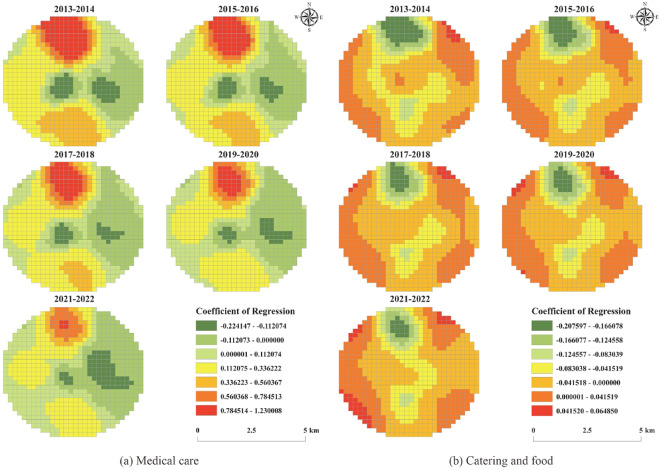
Cardiovascular disease (CVD) has become a significant threat to the health of urban populations, and the urban built environment, as a key determinant of cardiovascular health, affects residents through various dimensions including physical activity, urban pollution, mental health, and dietary habits. However, existing research predominantly focuses on macro-level geographic scales, with limited exploration of the potential impact of intra-urban microenvironments on CVD. This study focuses on the central area of Nanning, China, as the case study area, employing methods such as global spatial autocorrelation analysis, emerging spatiotemporal hotspot analysis, and spatiotemporal geographically weighted regression (GTWR) analysis to comprehensively examine the spatiotemporal associations between CVD and built environment elements. The results reveal that CVD and built environment elements exhibit significant spatial clustering and correlations, with all variables demonstrating spatial clustering patterns. Six built environment factors-parks and squares, transportation facilities, life services, sports and leisure, medical care, and Catering and food-are spatially associated with disease incidence. The influence of built environment factors on CVD varies and exhibits pronounced spatiotemporal heterogeneity, with the greatest coefficient fluctuation observed for parks and squares, and the smallest for catering services. Parks and squares generally contribute positively to cardiovascular health by lowering disease risk across most areas, although in the central zone, dense population and heavy traffic lead to a positive association with disease incidence. Fortunately, this adverse impact has been gradually mitigated through ongoing improvements in urban green space planning; transportation facilities increases disease risk due to associated noise and air pollution, with particularly strong effects observed in the central region. However, the implementation of green transportation initiatives has effectively mitigated this negative impact; life services show a positive association with CVD, but their diverse types and spatially balanced distribution render their impact relatively minor; sports and leisure are associated with reduced disease risk in the central part of the study area, but in the northeast and northwest, they exhibit a positive association due to population dispersion. As residents' usage habits become more consistent, the associated impacts are gradually stabilizing; medical care help reduce disease risk in the central and eastern regions, but show a positive correlation in the northern area due to patient overflow and referral patterns. With the more equitable distribution of healthcare resources, this relationship is gradually stabilizing; catering and food are positively associated with CVD, but the effect is relatively small and spatially balanced, likely due to their widespread and uniform distribution. These findings offer valuable case-based evidence for urban planning and public health policymaking, thereby contributing to the construction and advancement of healthy cities.
Keywords: Built environment; Cardiovascular diseases; Spatiotemporal epidemiology; Spatiotemporal evolution.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval and consent to participate: Our study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki, as well as relevant national and institutional guidelines for human research. Ethical approval was granted by the Medical Ethics Committee of Guangxi Ethnic Hospital (Approval No.: 2024-65). We accessed and analyzed de-identified cardiovascular department records with authorization from Guangxi Ethnic Hospital. These data were collected and maintained in accordance with the hospital’s patient data management policies and procedures. As this study involves only a retrospective analysis of existing medical records, without any direct patient interaction or risk of substantial harm, the Medical Ethics Committee of Guangxi Ethnic Hospital determined that individual patient consent was waived. Nonetheless, we ensured that all data used in the study were fully anonymized and protected, adhering to the highest standards of confidentiality and privacy.
Figures
References
-
- Roth, G. A., Mensah, G. A. & Fuster, V. Vol. 76 2980–2981 (American College of Cardiology Foundation Washington DC, (2020). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
