

Comparison of pregnancy outcomes between induction of labor at 40 weeks and 41 weeks in low-risk women with Singleton pregnancies: a retrospective cohort study
- PMID: 40382564
- PMCID: PMC12085817
- DOI: 10.1186/s12884-025-07691-0
Comparison of pregnancy outcomes between induction of labor at 40 weeks and 41 weeks in low-risk women with Singleton pregnancies: a retrospective cohort study
Abstract
Background: The best timing of delivery for term pregnancies has not been determined. This retrospective cohort study compared pregnancy outcomes between induction of labor (IOL) at 40 weeks and 41 weeks in low-risk women with singleton pregnancies and investigated maternal motivations regarding elective IOL.
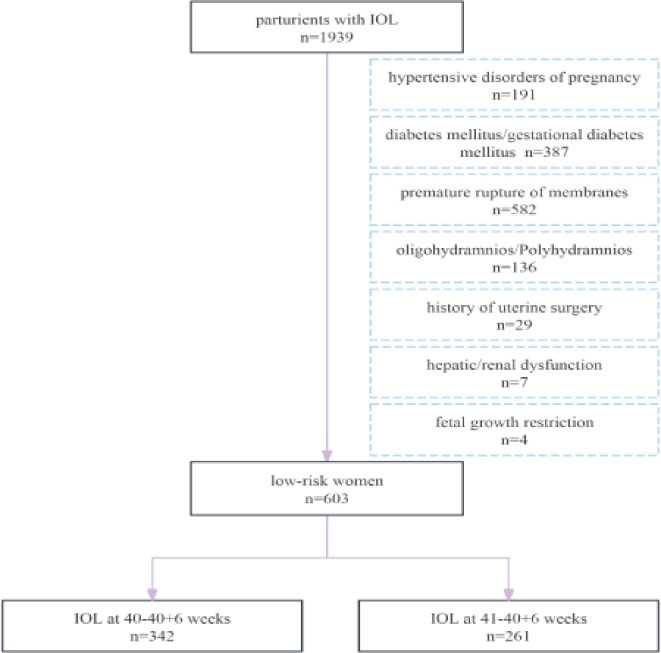
Methods: A total of 603 pregnant women were included in this study, with 342 (56.7%) undergoing IOL at 40-40+ 6 weeks and 261 (43.3%) at 41-41+ 6 weeks. The primary pregnancy outcome was the rate of cesarean section (CS), and the secondary pregnancy outcomes included the rates of neonatal asphyxia and neonatal intensive care unit (NICU) admission. Maternal motivations regarding elective IOL were investigated.
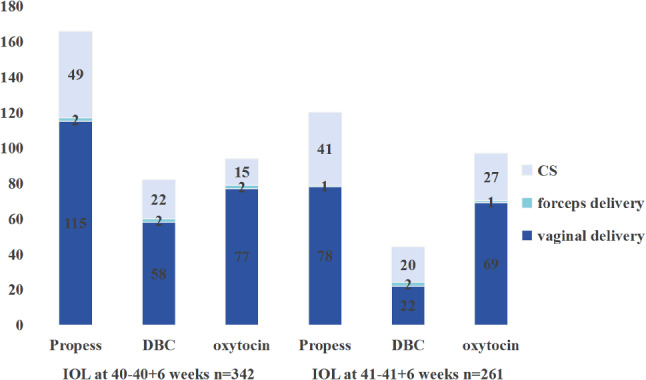
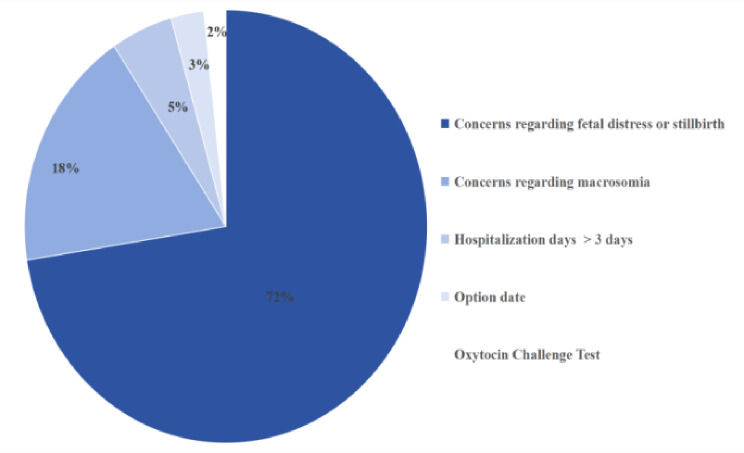
Results: The rate of CS was 25.1% in the IOL at 40-40+ 6 weeks group and 33.7% in the IOL at 41-41+ 6 weeks group (p = 0.021). The three most prevalent indications for CS in both groups were: (1) non-reassuring fetal heart rate patterns (NRFHRP); (2) meconium-stained amniotic fluid; and (3) failed induction of labor. Compared with the 41-week IOL group, women who underwent IOL at 40 weeks' gestation exhibited higher educational attainment (93.6% vs. 82.0%, P < 0.001), a higher proportion of high-income families (91.5% vs. 68.2%, P < 0.001), a higher proportion of multiparae (24.0% vs. 16.5%, P < 0.05), a lower proportion of ripeness of the cervix (27.5% vs. 37.2%, P < 0.05), shorter hospitalization durations (5.84 ± 1.79 vs. 6.17 ± 1.95, P < 0.05), and higher hospitalization costs (13627.39 ± 3227.56 vs. 10837.77 ± 3276.73, P < 0.001). No significant intergroup differences were observed in the rates of neonatal asphyxia and NICU admission. The most common motivation for elective IOL was concern regarding fetal distress or stillbirth. Parity ≥ 1 and a Bishop score ≥ 6 were protective factors against CS following IOL.
Conclusions: IOL at 40 weeks did not result in increased adverse outcomes compared to IOL at 41 weeks. Parturients with higher education and income were more likely to choose elective IOL. Parity ≥ 1 and a Bishop score ≥ 6 were protective factors against CS following IOL. These may provide a new option for clinical decision-making.
Keywords: Maternal motivation; Pregnancy outcomes; Rate of cesarean section; Time of induction of labor.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study involving participants was reviewed and approved by the institutional review board of the Maternal and Child Health Hospital of Hubei Province and was based on the principles of the Declaration of Helsinki. All subjects provided written Informed consent for participation. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Maternal and newborn outcomes with elective induction of labor at term.Am J Obstet Gynecol. 2019 Mar;220(3):273.e1-273.e11. doi: 10.1016/j.ajog.2019.01.223. Epub 2019 Feb 17. Am J Obstet Gynecol. 2019. PMID: 30716284
-
Timing of induction of labor in suspected macrosomia: retrospective cohort study, systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2024 Oct;64(4):443-452. doi: 10.1002/uog.27643. Ultrasound Obstet Gynecol. 2024. PMID: 38477187
-
Induction of labor before 40 weeks is associated with lower rate of cesarean delivery in women with gestational diabetes mellitus.Am J Obstet Gynecol. 2016 Mar;214(3):364.e1-8. doi: 10.1016/j.ajog.2015.12.021. Am J Obstet Gynecol. 2016. PMID: 26928149
-
Outcomes among Nulliparous Women Undergoing Nonmedically Indicated Induction of Labor at 39 Weeks Compared with Expectant Management Differ by Maternal Age.Am J Perinatol. 2024 May;41(S 01):e1061-e1068. doi: 10.1055/a-1990-8411. Epub 2022 Nov 30. Am J Perinatol. 2024. PMID: 36452970
-
Elective induction of labor at 39 weeks compared with expectant management: a meta-analysis of cohort studies.Am J Obstet Gynecol. 2019 Oct;221(4):304-310. doi: 10.1016/j.ajog.2019.02.046. Epub 2019 Feb 25. Am J Obstet Gynecol. 2019. PMID: 30817905
References
-
- Khambalia AZ, Roberts CL, Nguyen M, et al. Predicting date of birth and examining the best time to date a pregnancy. Int J Gynaecol Obstet. 2013;123:105–9. - PubMed
-
- Garriga M, Van’t Hooft J. When is the right time to induce labour? BMJ Evid Based Med. 2021;26(3):135–6. - PubMed
-
- Grobman WA. The role of labor induction in modern obstetrics. Am J Obstet Gynecol. 2024;230(3S):S662–8. - PubMed
-
- Martin JA, Hamilton BE, Sutton PD, et al. Births: final data for 2008. Natl Vital Stat Rep. 2010;59(1):1–71. - PubMed
-
- WHO recommendations on mechanical methods for induction of labour. Geneva: World Health Organization; 2022. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
