

Meta-analysis of the optimal needle length and decompression site for tension pneumothorax and consensus recommendations on current ATLS and ETC guidelines
- PMID: 40383767
- PMCID: PMC12087068
- DOI: 10.1186/s13017-025-00613-7
Meta-analysis of the optimal needle length and decompression site for tension pneumothorax and consensus recommendations on current ATLS and ETC guidelines
Abstract
Background: Tension pneumothorax (TP) is a life-threatening condition. The immediate recommended management is needle decompression (ND), followed by the insertion of an intercostal chest drain. The European Trauma Course (ETC) and the Advanced Trauma Life Support (ATLS) guidelines differ on needle size and decompression site, creating clinical uncertainty. This meta-analysis aims to explore the optimal approach for emergency needle decompression in TP.
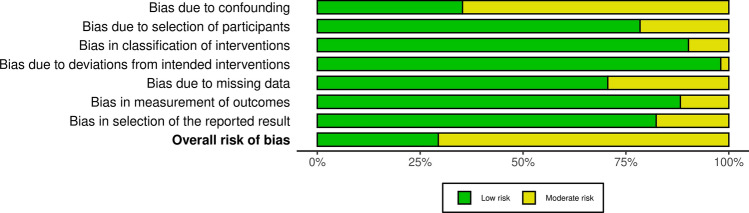
Methods: This meta-analysis followed the PRISMA 2020 guidelines. It included English-language RCTs, cohort, case-control, cross-sectional studies, and case series with more than six patients. Studies on adults undergoing needle decompression therapy for TP or with chest wall thickness measurements were included. Ovid MEDLINE, Embase, and Web of Science databases were searched until May 31, 2024. Data were extracted, assessed for quality using OCEBM and GRADE, and analyzed using SPSS and OpenMeta with random-effects models.
Primary outcome: needle decompression failure rate.
Secondary outcomes: patient demographics, cannula size, and chest wall thickness comparisons.
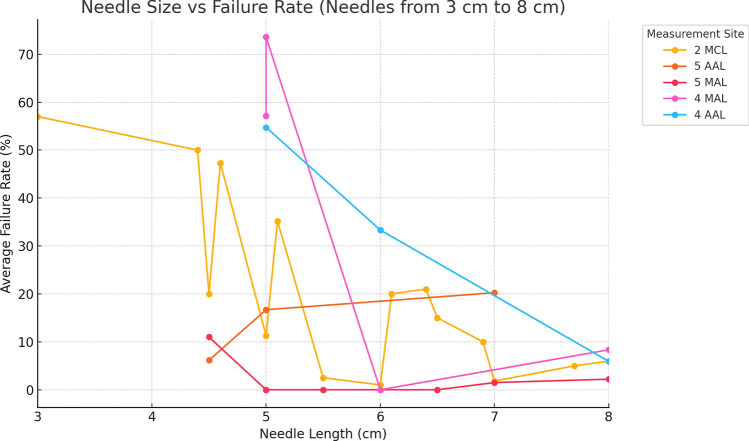
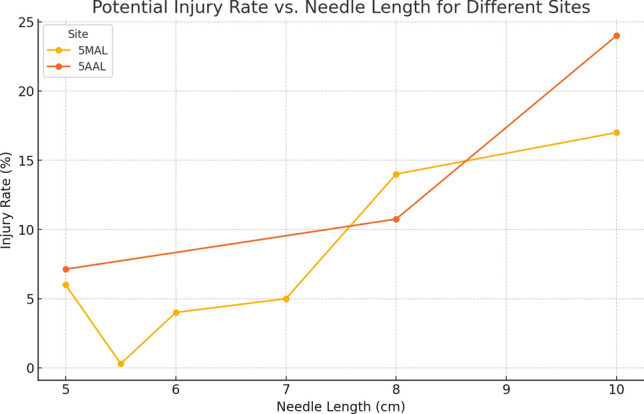
Results: This review analyzed 51 studies on needle decompression for TP, with a weighted mean patient age of 36.67 years. Radiological data from 24 studies (n = 8046) indicated a 32.84% failure rate for needle penetration into the pleural cavity (I2: 99.72%). Increased needle length reduced failure rates by 7.76% per cm. No significant differences in chest wall thickness between genders were observed (T-test, p = 0.77), but thickness at the 5th anterior axillary line (5AAL) and 5th midaxillary line (5MAL) was less than at the 2nd midclavicular line (2MCL). Injury rates were higher at 5AAL than 5MAL, with strong positive correlations between needle length and injury at these sites (0.88, 0.91).
Conclusion: Based on our meta-analysis, a 7 cm needle may be appropriate for decompression of right-sided tension pneumothorax at either the 5th intercostal space along the midaxillary line or the 2nd intercostal space along the midclavicular line. For left-sided cases, given the potential risk of cardiac injury, the 2nd midclavicular line is a safer option. However, these recommendations should be interpreted with caution due to considerable heterogeneity among the included studies, potential risk of bias, and variability in measurement techniques. Clinical decisions should always be individualized, taking into account patient-specific factors.
Keywords: Chest wall thickness; Iatrogenic injury; Intercostal space; Needle decompression; Needle length; Tension pneumothorax; Trauma care.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: No ethical approvals are required for this study. Patients and public involvement: No patients were involved in this study as it is a meta-analysis. Consent for publication: All authors consent for this version of the paper to be published. Competing interests: The authors declare no competing interests.
Figures





References
-
- Jain V, Bordes S, Bhardwaj A. Physiology, Pulmonary Circulatory System. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 http://www.ncbi.nlm.nih.gov/books/NBK525948/. Accessed 6 May 2022 - PubMed
-
- Schmidt RF, Lang F, Heckmann M. Physiologie des Menschen mit Pathophysiologie: mit Online-Repetitorium. Cham: Springer; 2017.
-
- Surgeons AC of. Committee on Trauma: Advanced Trauma Life Support. Student Course Manual. ACS Chicago; 2018.
-
- Jalota Sahota R, Sayad E. Tension Pneumothorax. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 [cited 2022 May 6]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK559090/
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
