

Single-cell transcriptomic characterization of microscopic colitis
- PMID: 40383833
- PMCID: PMC12086216
- DOI: 10.1038/s41467-025-59648-8
Single-cell transcriptomic characterization of microscopic colitis
Abstract
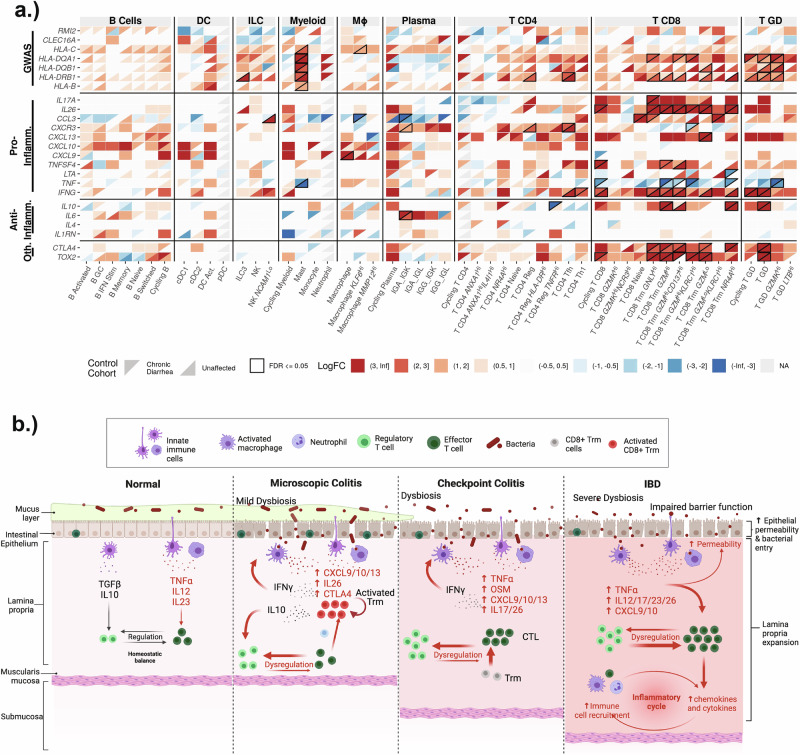
Microscopic colitis (MC) is a chronic inflammatory disease of the large intestine and a common cause of chronic diarrhea in older adults. Here, we use single-cell RNA sequencing analysis of colonic mucosal tissue to build a cellular and molecular model for MC. Our results show that in MC, there is a substantial expansion of tissue CD8+ T cells, likely arising from local expansion following T cell receptor engagement. Within the T cell compartment, MC is characterized by a shift in CD8 tissue-resident memory T cells towards a highly cytotoxic and inflammatory phenotype and expansion of CD4+ T regulatory cells. These results provide insight into inflammatory cytokines shaping MC pathogenesis and highlight notable similarities and differences with other immune-mediated intestinal diseases, including a common upregulation of IL26 and an MC-specific upregulation of IL10. These data help identify targets against enteric T cell subsets as an effective strategy for treatment of MC.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Hamed Khalili has received consulting fees from Aditium Bio and currently serves on the clinical advisory board of Cylinder Health. A.C.V. has a financial interest in 10X Genomics. 10X Genomics designs and manufactures gene sequencing technology for use in research, and such technology is being used in this research; these interests were reviewed by The Massachusetts General Hospital and Mass General Brigham in accordance with their institutional policies. The remaining authors declare no competing interests.
Figures





References
-
- Khalili, H. et al. Mortality of patients with microscopic colitis in Sweden. Clin. Gastroenterol. Hepatol.18, 2491–2499.e3 (2020). - PubMed
-
- Nyhlin, N., Wickbom, A., Montgomery, S. M., Tysk, C. & Bohr, J. Long-term prognosis of clinical symptoms and health-related quality of life in microscopic colitis: a case-control study. Aliment Pharm. Ther.39, 963–972 (2014). - PubMed
-
- Guagnozzi, D., Lucendo, A. J., Angueira-Lapeña, T., González-Castillo, S. & Tenias Burillo, J. M. Prevalence and incidence of microscopic colitis in patients with diarrhoea of unknown aetiology in a region in central Spain. Dig. Liver Dis.44, 384–388 (2012). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
