

Machine Learning for the Prediction of Acute Kidney Injury in Critically Ill Patients With Coronary Heart Disease: Algorithm Development and Validation
- PMID: 40383933
- PMCID: PMC12159552
- DOI: 10.2196/72349
Machine Learning for the Prediction of Acute Kidney Injury in Critically Ill Patients With Coronary Heart Disease: Algorithm Development and Validation
Abstract
Background: Acute kidney injury (AKI) frequently occurs in critically ill patients with coronary heart disease (CHD), and its development markedly elevates mortality rates and prolongs hospitalization duration. Early AKI prediction is crucial for timely intervention and amelioration of patient outcomes.
Objective: This study aimed to develop and verify a clinical prediction model for the occurrence of AKI upon admission in the critically ill population with CHD through machine learning (ML).
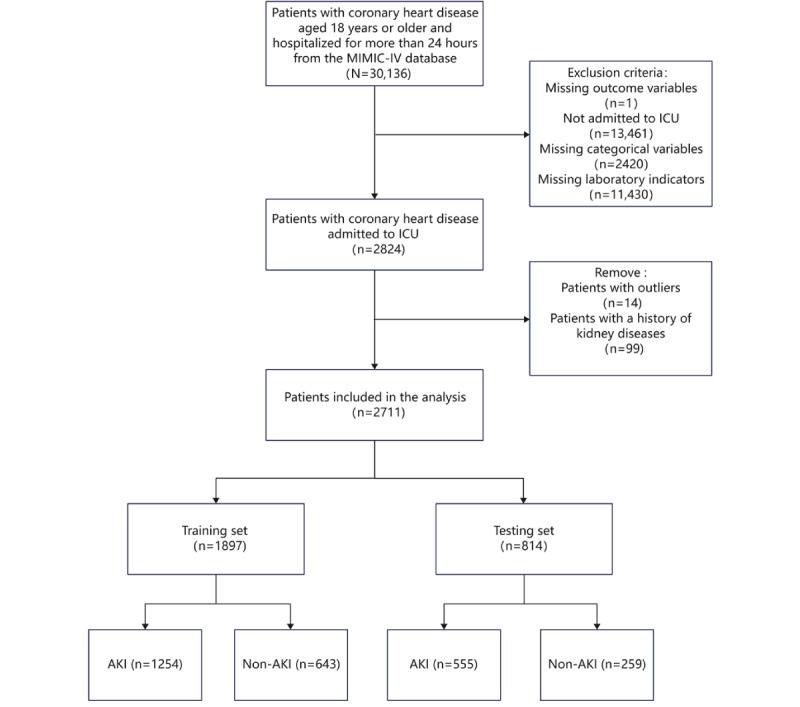
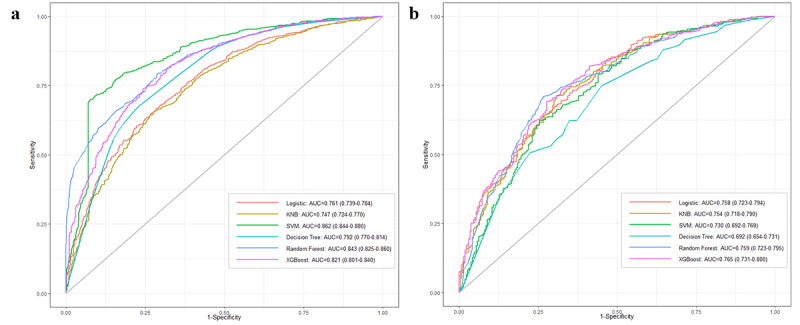
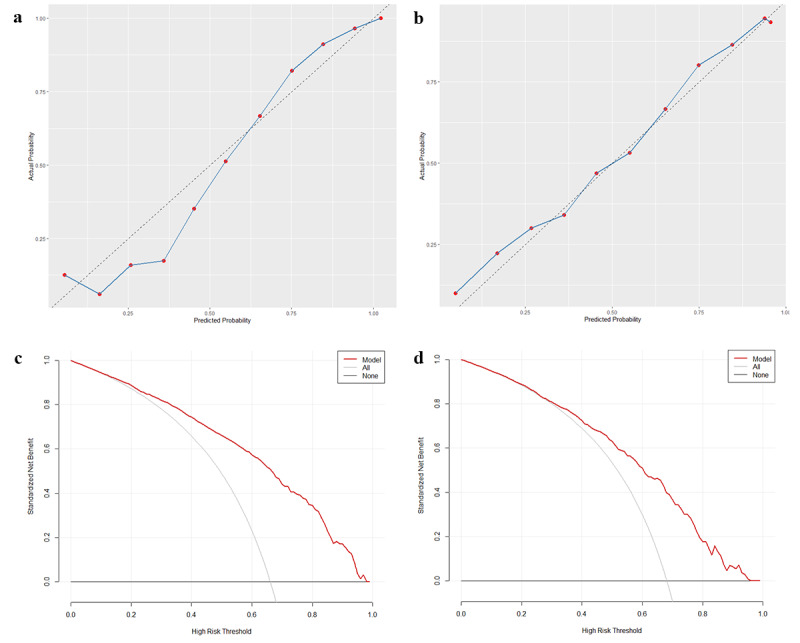
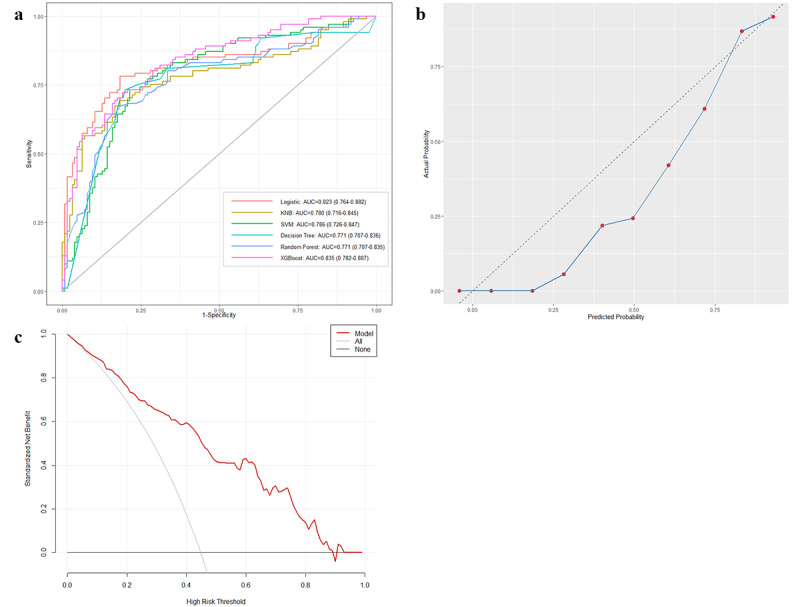
Methods: Data from the MIMIC-IV (Medical Information Mart for Intensive Care IV) version 2.2 database were gathered and included information about critically ill individuals with CHD in the intensive care unit (ICU). The dataset was randomized into a training set (70%) and a testing set (30%). Least absolute shrinkage and selection operator (LASSO) regression was used for feature variable selection. ML models, including logistic regression (LR), decision tree (DT), naive Bayes (NB), random forest (RF), extreme gradient boosting (XGBoost), and support vector machine (SVM), were constructed using 13 variables in the training set. The 6 models were compared in the testing set to identify the best-performing model. Subsequently, the model was assessed using calibration curve analysis and decision curve analysis (DCA). External validation was conducted using data from the Second Affiliated Hospital of Zhengzhou University. Ultimately, the predictive model was interpreted via Shapley Additive Explanation (SHAP) values.
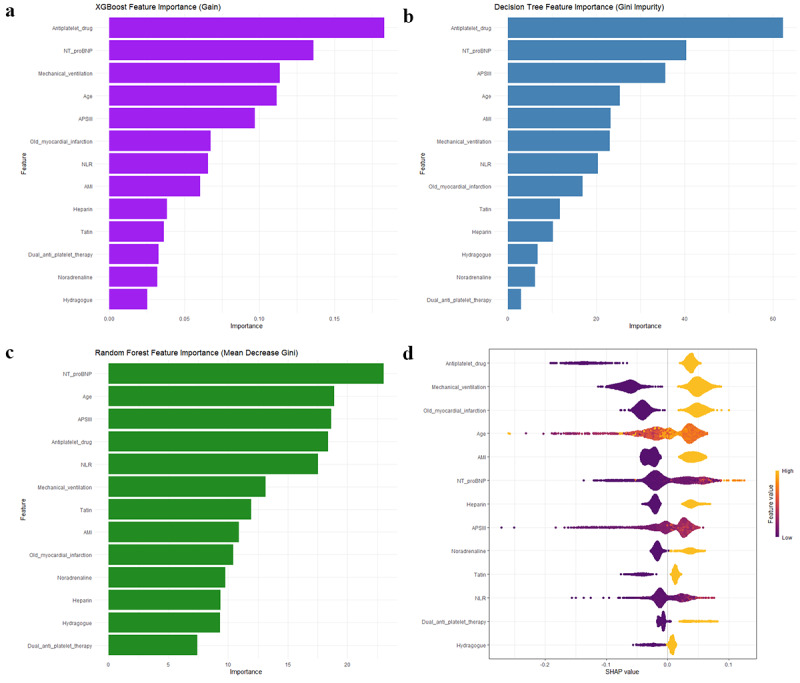
Results: In total, 2711 patients with CHD admitted to the ICU were selected, with 1809 (66.7%) having AKI. XGBoost exhibited the best performance regarding discrimination (area under the receiver operating characteristic curve [AUROC]=0.765, 95% CI 0.731-0.800), accuracy (0.725), and sensitivity (0.759). External validation using a cohort of 226 patients confirmed the strong generalizability of the XGBoost model (AUROC=0.835, 95% CI 0.782-0.887). Feature importance analyses derived from SHAP values, DT, RF, and XGBoost consistently identified 5 key predictors associated with the development of AKI: mechanical ventilation, use of antiplatelet agents, age, N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels, and acute physiology score III (APSIII).
Conclusions: ML models can serve as reliable tools for forecasting AKI in the critically ill population with CHD. The XGBoost model is highly accurate and may aid doctors in identifying high-risk individuals for early intervention to lower mortality.
Keywords: MIMIC-IV database; acute kidney injury; coronary artery disease; coronary heart disease; machine learning.
©Yike Li, Mingyang Xiao, Yaqian Li, Lulu Lv, Shanshan Zhang, Yuhui Liu, Juan Zhang. Originally published in JMIR Medical Informatics (https://medinform.jmir.org), 28.05.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

Similar articles
-
Construction and evaluation of a mortality prediction model for patients with acute kidney injury undergoing continuous renal replacement therapy based on machine learning algorithms.Ann Med. 2024 Dec;56(1):2388709. doi: 10.1080/07853890.2024.2388709. Epub 2024 Aug 19. Ann Med. 2024. PMID: 39155811 Free PMC article.
-
Construction and validation of prognostic models in critically Ill patients with sepsis-associated acute kidney injury: interpretable machine learning approach.J Transl Med. 2023 Jun 22;21(1):406. doi: 10.1186/s12967-023-04205-4. J Transl Med. 2023. PMID: 37349774 Free PMC article.
-
AKIMLpred: An interpretable machine learning model for predicting acute kidney injury within seven days in critically ill patients based on a prospective cohort study.Clin Chim Acta. 2024 Jun 1;559:119705. doi: 10.1016/j.cca.2024.119705. Epub 2024 May 1. Clin Chim Acta. 2024. PMID: 38702035
-
Predicting renal function recovery and short-term reversibility among acute kidney injury patients in the ICU: comparison of machine learning methods and conventional regression.Ren Fail. 2022 Dec;44(1):1326-1337. doi: 10.1080/0886022X.2022.2107542. Ren Fail. 2022. PMID: 35930309 Free PMC article. Review.
-
Methodological Review of Classification Trees for Risk Stratification: An Application Example in the Obesity Paradox.Nutrients. 2025 May 31;17(11):1903. doi: 10.3390/nu17111903. Nutrients. 2025. PMID: 40507172 Free PMC article. Review.
References
-
- Bagur R, Webb JG, Nietlispach F, Dumont E, De Larochellière R, Doyle D, Masson J, Gutiérrez MJ, Clavel M, Bertrand OF, Pibarot P, Rodés-Cabau J. Acute kidney injury following transcatheter aortic valve implantation: predictive factors, prognostic value, and comparison with surgical aortic valve replacement. Eur Heart J. 2010 Apr;31(7):865–74. doi: 10.1093/eurheartj/ehp552. https://europepmc.org/abstract/MED/20037180 ehp552 - DOI - PMC - PubMed
-
- Schiefer J, Bernardi MH, Lichtenegger P, Schak G, Atallah L, Ristl R, Ramazanova D, Faybik P. Incidence and outcomes of AKI in postoperative patients admitted to ICU using full KDIGO criteria - a cohort study. J Clin Anesth. 2023 Oct;89:111156. doi: 10.1016/j.jclinane.2023.111156. https://linkinghub.elsevier.com/retrieve/pii/S0952-8180(23)00106-X S0952-8180(23)00106-X - DOI - PubMed
-
- Ma K, Li J, Shen G, Zheng D, Xuan Y, Lu Y, Li W. Development and validation of a risk nomogram model for predicting contrast-induced acute kidney injury in patients with non-ST-elevation acute coronary syndrome undergoing primary percutaneous coronary intervention. Clin Interv Aging. 2022;17:65–77. doi: 10.2147/CIA.S349159. https://www.tandfonline.com/doi/abs/10.2147/CIA.S349159?url_ver=Z39.88-2... 349159 - DOI - DOI - PMC - PubMed
-
- Peng X, Li L, Wang X, Zhang H. A machine learning-based prediction model for acute kidney injury in patients with congestive heart failure. Front Cardiovasc Med. 2022 Mar 4;9:842873. doi: 10.3389/fcvm.2022.842873. https://europepmc.org/abstract/MED/35310995 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
