

Hematomyelia after epidural anesthesia: a rare complication with putative multifactorial and occult etiology
- PMID: 40384194
- PMCID: PMC12236289
- DOI: 10.47162/RJME.66.1.07
Hematomyelia after epidural anesthesia: a rare complication with putative multifactorial and occult etiology
Abstract
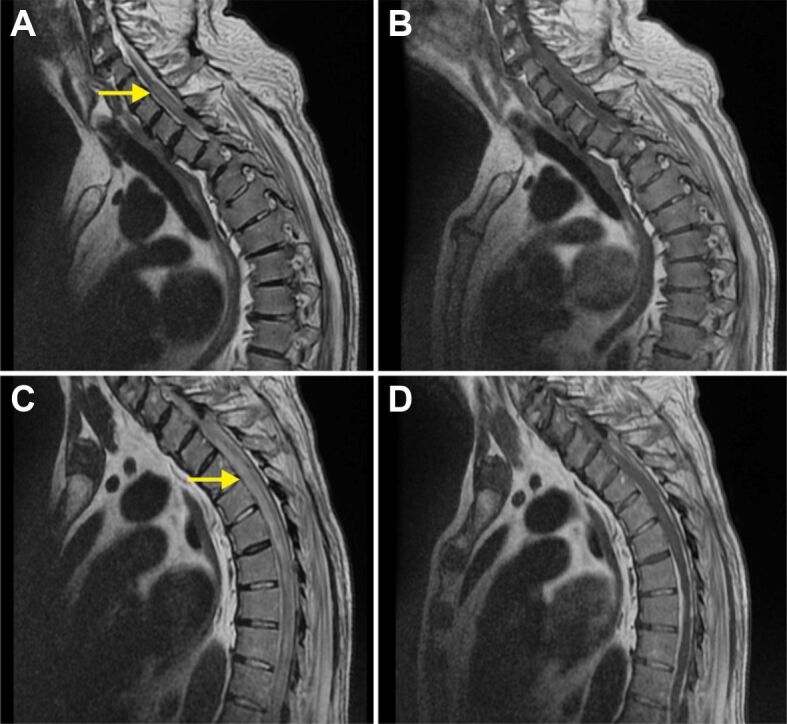
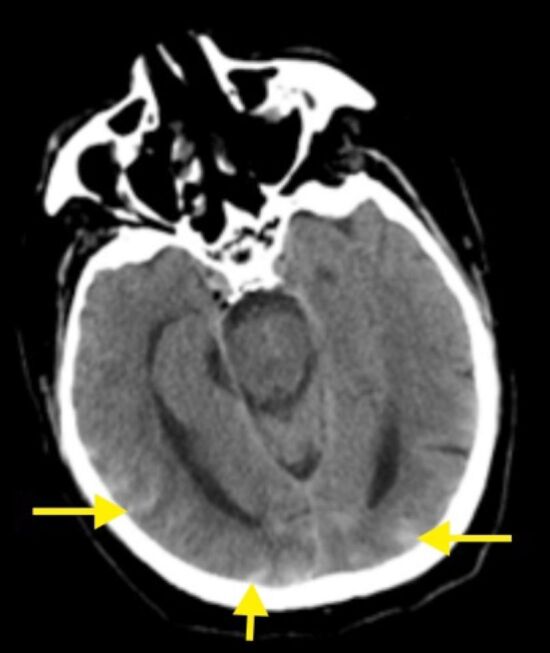
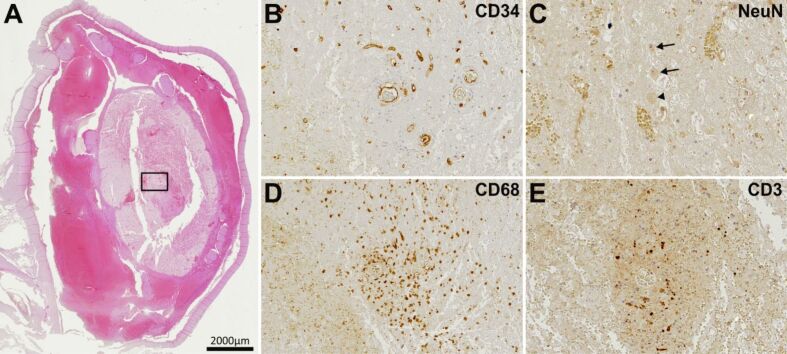
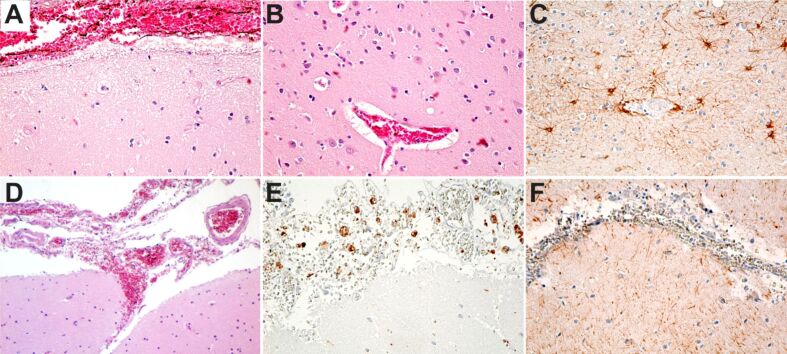
Subarachnoid hemorrhage (SAH) and spinal hematomas are considered serious but rare complications of spinal pathology. They occur after spinal anesthesia, especially in patients with risk factors such as autoimmune diseases, blood coagulation pathology, anticoagulant treatment, vascular malformations, intramedullary or spinal cord tumors, or can be multifactorial. Usually, anticoagulant therapy represents an additional factor regarding spinal SAH (SSAH) or spinal hematomas. None of the direct oral anticoagulants has a higher chance of producing a spinal hemorrhage. The diagnosis can be established based on the clinical picture of SSAH or myelopathy syndrome, completed with magnetic resonance imaging (MRI). In this study, we present the latest data from the literature regarding SSAH and hematomas and compare them with the data of a 77-year-old man with a history of atrial fibrillation, on oral anticoagulant treatment, who developed a SSAH and spinal hematoma after elective surgery for an inguinal hernia.
Keywords: hematomyelia; regional anesthesia; subdural hematoma.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures
Similar articles
-
Use of platelet transfusions prior to lumbar punctures or epidural anaesthesia for the prevention of complications in people with thrombocytopenia.Cochrane Database Syst Rev. 2018 Apr 30;4(4):CD011980. doi: 10.1002/14651858.CD011980.pub3. Cochrane Database Syst Rev. 2018. PMID: 29709077 Free PMC article.
-
Paravertebral block versus thoracic epidural for patients undergoing thoracotomy.Cochrane Database Syst Rev. 2016 Feb 21;2(2):CD009121. doi: 10.1002/14651858.CD009121.pub2. Cochrane Database Syst Rev. 2016. PMID: 26897642 Free PMC article.
-
Uncommon Non-MS Demyelinating Disorders of the Central Nervous System.Curr Neurol Neurosci Rep. 2025 Jul 1;25(1):45. doi: 10.1007/s11910-025-01432-8. Curr Neurol Neurosci Rep. 2025. PMID: 40591029 Review.
-
Epidural therapy for the treatment of severe pre-eclampsia in non labouring women.Cochrane Database Syst Rev. 2017 Nov 28;11(11):CD009540. doi: 10.1002/14651858.CD009540.pub2. Cochrane Database Syst Rev. 2017. PMID: 29181841 Free PMC article.
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
