

The role of CDX2, MUC5AC, and p53 in the evaluation of the progression of serrated lesions toward colorectal carcinoma
- PMID: 40384196
- PMCID: PMC12236287
- DOI: 10.47162/RJME.66.1.09
The role of CDX2, MUC5AC, and p53 in the evaluation of the progression of serrated lesions toward colorectal carcinoma
Abstract
Background: Serrated colorectal lesions represent a potential precursor of 15-30% of colorectal carcinoma, although the exact mechanisms are not fully understood. The serrated pathway of colorectal carcinogenesis may be correlated with gastric-type metaplasia of the colon and modified expression of caudal type homeobox 2 (CDX2) and local mucins (MUCs).
Patients, materials and methods: We performed a retrospective study of patients with resected polyps during 2014-2021. The prevalence of serrated lesions, risk factors associated with malignant polyps, and the role of gastric-type metaplasia associated with serrated pathway of carcinogenesis (CDX2, MUC5AC) and of p53 immunostaining in serrated lesions with dysplasia and carcinoma were assessed.
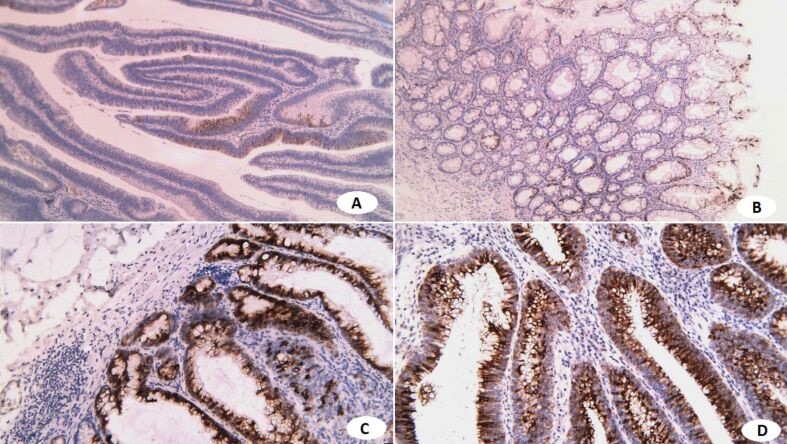
Results: Five hundred twenty two (522) patients had 1199 polyps removed. We noted a 12.8% prevalence of sessile serrated adenoma∕polyps (SSA∕P) and traditional serrated adenomas (TSA); 17.4% had hyperplastic polyps. The malignancy rate of resected polyps was higher in tubulovillous adenoma (TVA) and villous adenoma (12.3-20%) than in SSA∕P (8.3%) and TSA (4.8%). In TSA, no significant associations between malignancy and age, gender, size, location, or endoscopic appearance were noted. In SSA∕P, malignant polyps were much larger, especially for the right side lesions, but the macroscopic type was not correlated with malignancy risk. Immunohistochemistry (IHC) was performed in 26 polyps with dysplasia or carcinoma; all cases had CDX2 immunostaining in the tumor cell's nucleus, with an average percentage of 96.5%. MUC5AC immunostaining was identified in the tumor cells' cytoplasm, with an average percentage of 31.81%; the intensity reaction was variable (average score 4.5). The percentage, intensity, and score for CDX2 IHC were similar for TSA and TVA and were lower for SSA∕P with low-grade dysplasia (LGD), while for SSA∕P with high-grade dysplasia (HGD) or carcinoma in situ (CIS), the percentage, intensity, and score were similar to TSA and TVA. p53 immunostaining was also positive in all cases, with an average percentage of 50.95% in the tumor cells' nucleus. p53 and MUC5AC had increased percentage, intensity, and scores from LGD to HGD in SSA∕P and decreased mean percentage, intensity, and scores in TSA and TVA.
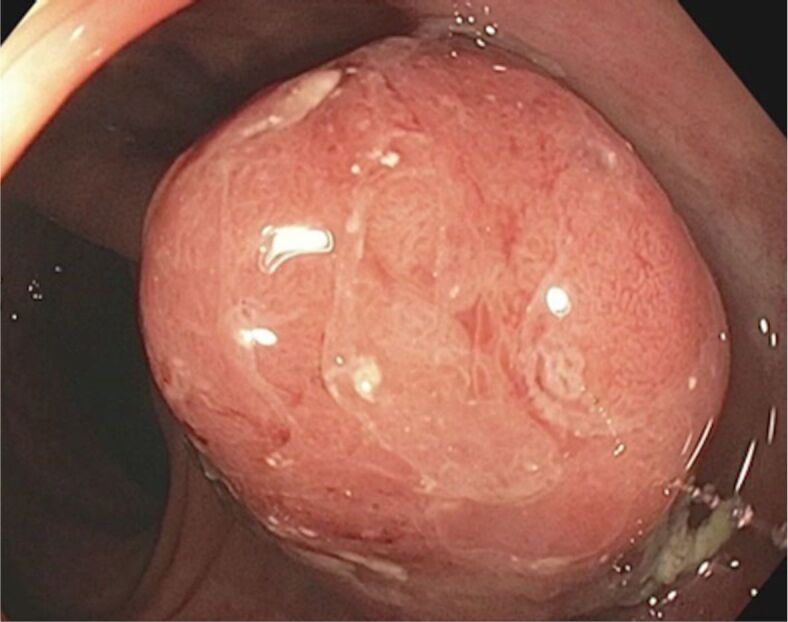
Conclusions: The risk of malignancy in serrated lesions seems lower than in conventional adenomas, however, sessile serrated lesions can be involved in the appearance of interval cancers because of flat and pale macroscopic aspects. Gastric-type intestinal metaplasia may be associated with the serrated pathway, but more studies are needed to clarify mechanisms associated with serrated carcinogenesis.
Keywords: CDX2; MUC5AC; malignant polyp; p53; serrated lesion.
Conflict of interest statement
The authors declare no conflict of interests.
Figures







References
-
- Sakai E, Fukuyo M, Ohata K, Matsusaka K, Doi N, Mano Y, Takane K, Abe H, Yagi K, Matsuhashi N, Fukushima J, Fukayama M, Akagi K, Aburatani H, Nakajima A, Kaneda A. Genetic and epigenetic aberrations occurring in colorectal tumors associated with serrated pathway. Int J Cancer. 2016;138(7):1634–1644. - PMC - PubMed
-
- Herreros de, González-Lois C, Santiago J. Serrated lesions and serrated polyposis syndrome. Rev Esp Enferm Dig. 2017;109(7):516–526. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
