

Impact of Dexmedetomidine on Analgesia and Inflammatory Response in Knee Surgery: A Study of IPACK and ACB Techniques
- PMID: 40384422
- PMCID: PMC12080283
- DOI: 10.12659/MSM.947087
Impact of Dexmedetomidine on Analgesia and Inflammatory Response in Knee Surgery: A Study of IPACK and ACB Techniques
Abstract
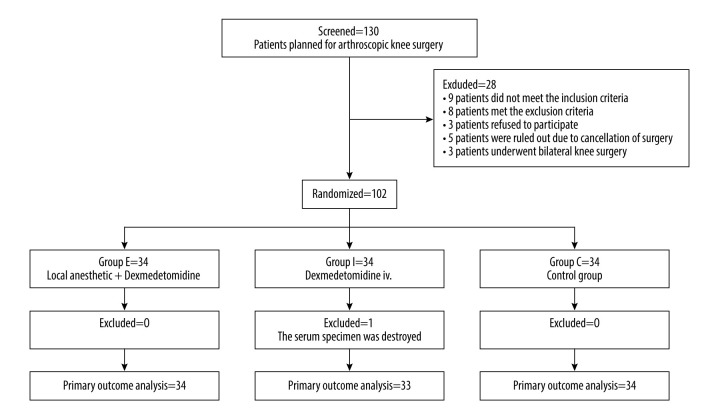
BACKGROUND The interspace between the popliteal artery and posterior capsule of the knee block (IPACK) combined with adductor canal block (ACB) has short-term analgesic effect after arthroscopic knee surgery(AKS), and prolonging the duration of analgesia is very important for patients to recover quickly after surgery. The purpose of this study was to investigate whether perineural dexmedetomidine (DEX) or intravenous can prolong the analgesic time of IPACK and ACB, and ultimately promote the postoperative rehabilitation of patients undergoing AKS. MATERIAL AND METHODS In this randomized controlled trial, 102 eligible AKS patients were allocated to 3 groups: perineural DEX with ropivacaine for Group E (n=34), intravenous DEX for Group I (n=34), and standard IPACK-ACB (ropivacaine alone) for Group C (n=34). The outcomes included resting and active Visual Analog Scale (VAS) scores at 6 h, 12 h, 24 h, 48 h, 54 h, and 60 h postoperatively, inflammatory marker levels on the first postoperative day, and maximum walking distance at 24 and 48 hours after surgery. RESULTS There were no significant demographic differences between the 3 groups. Resting and active VAS scores in Group E were significantly lower than those in Group C within 48 hours postoperatively (P<0.05), VAS at 48 h resting state (P<0.001, mean difference,-1.15; 95% CI, -1.65 to -0.65), VAS at 48 h active state (P<0.001, mean difference,-0.91; 95% CI, -1.32 to -0.50). On the first postoperative day, IL-1β levels in Groups E and I were significantly lower than in Group C (P<0.05). Group E had a significantly longer maximum walking distance at 24 and 48 hours after surgery compared to Groups I and C (P<0.001). CONCLUSIONS Perineural DEX prolongs IPACK-ACB analgesia to 48 hours, improves functional recovery, and attenuates IL-1β release, outperforming intravenous administration. These findings support the integration of route-specific DEX into enhanced recovery protocols for AKS.
Conflict of interest statement
Figures



Similar articles
-
Enhanced Postoperative Pain Management and Mobility Following Arthroscopic Knee Surgery: A Comparative Study of Adductor Canal Block with and without IPACK Block.Med Sci Monit. 2024 Jul 28;30:e943735. doi: 10.12659/MSM.943735. Med Sci Monit. 2024. PMID: 39068511 Free PMC article. Clinical Trial.
-
Continuous adductor canal block is superior to adductor canal block alone or adductor canal block combined with IPACK block (interspace between the popliteal artery and the posterior capsule of knee) in postoperative analgesia and ambulation following total knee arthroplasty: randomized control trial.Musculoskelet Surg. 2022 Jun;106(2):155-162. doi: 10.1007/s12306-020-00682-8. Epub 2020 Sep 27. Musculoskelet Surg. 2022. PMID: 32980982 Clinical Trial.
-
Comparison of adductor canal block and IPACK block (interspace between the popliteal artery and the capsule of the posterior knee) with adductor canal block alone after total knee arthroplasty: a prospective control trial on pain and knee function in immediate postoperative period.Eur J Orthop Surg Traumatol. 2018 Oct;28(7):1391-1395. doi: 10.1007/s00590-018-2218-7. Epub 2018 May 2. Eur J Orthop Surg Traumatol. 2018. PMID: 29721648 Clinical Trial.
-
iPACK block (local anesthetic infiltration of the interspace between the popliteal artery and the posterior knee capsule) added to the adductor canal blocks versus the adductor canal blocks in the pain management after total knee arthroplasty: a systematic review and meta-analysis.J Orthop Surg Res. 2022 Aug 12;17(1):387. doi: 10.1186/s13018-022-03272-5. J Orthop Surg Res. 2022. PMID: 35962410 Free PMC article.
-
Does the Addition of iPACK Block to Adductor Canal Block Provide Improved Analgesic Effect in Total Knee Arthroplasty? A Systematic Review and Meta-Analysis.J Knee Surg. 2023 Mar;36(4):345-353. doi: 10.1055/s-0041-1733882. Epub 2021 Oct 2. J Knee Surg. 2023. PMID: 34600437
References
-
- Hussain N, Brull R, Vannabouathong C, et al. Analgesic effectiveness of motor-sparing nerve blocks for total knee arthroplasty: A network meta-analysis. Anesthesiology. 2023;139(4):444–61. - PubMed
-
- Restrepo-Holguin M, Kopp SL, Johnson RL. Motor-sparing peripheral nerve blocks for hip and knee surgery. Curr Opin Anaesthesiol. 2023;36(5):541–46. - PubMed
-
- Mou P, Wang D, Tang XM, et al. Adductor canal block combined with IPACK block for postoperative analgesia and function recovery following total knee arthroplasty: A prospective, double-blind, randomized controlled study. J Arthroplasty. 2022;37(2):259–66. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
