

Ultrasound evaluation of changes in endometrial receptivity from the day of ovulation to the day of transfer in patients with a history of intrauterine adhesions: a prospective cohort study
- PMID: 40384661
- PMCID: PMC12084758
- DOI: 10.21037/qims-24-2034
Ultrasound evaluation of changes in endometrial receptivity from the day of ovulation to the day of transfer in patients with a history of intrauterine adhesions: a prospective cohort study
Abstract
Background: High rates of infertility and pregnancy complications in patients with intrauterine adhesion (IUA) even after surgical repair may be associated with poor endometrial receptivity (ER). In our previous study, we found that changes occurred in ER from the day of ovulation to the day of transfer in patients with a normal uterine cavity during natural cycles. However, the changes in ER ultrasound indicators in patients with a history of IUA during natural cycles are unclear, and this study thus aimed to analyze these changes.
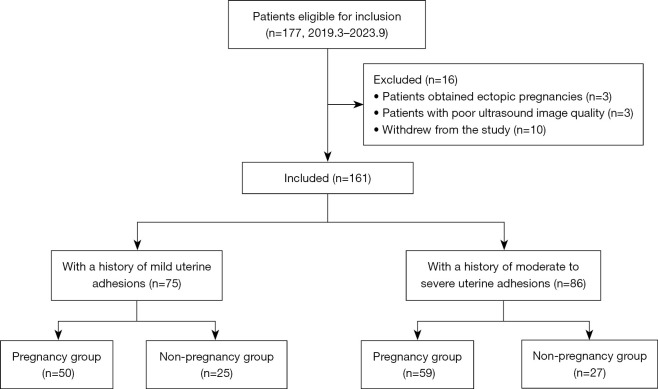
Methods: A prospective cohort study of 161 women with a history of IUA who underwent frozen-thawed embryo transfer (FET) was conducted. ER changes from ovulation to the transfer day in the overall, clinically pregnant, and nonpregnant populations were analyzed. Patients were further allocated to the mild IUA or moderate-to-severe IUA subgroup based on the degree of IUA.
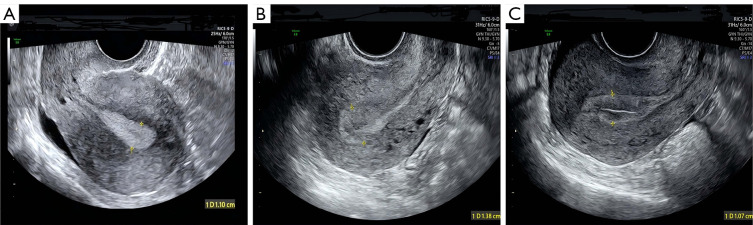
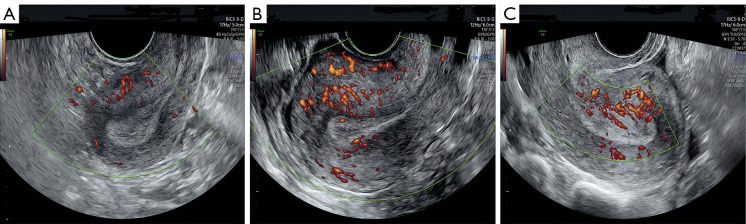
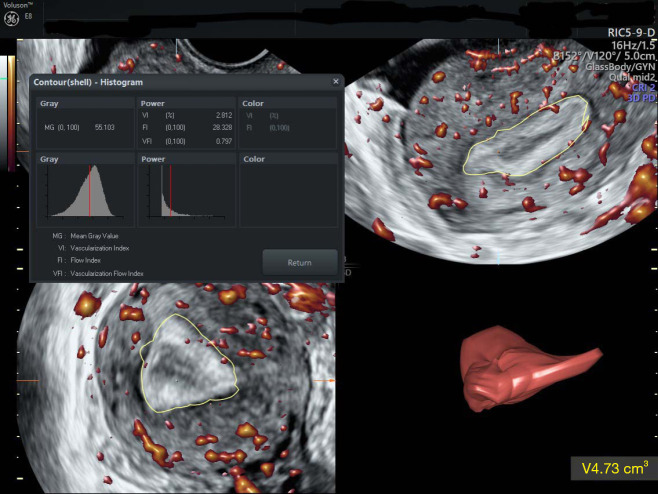
Results: Endometrial morphology was mainly type C (a "triple-line" endometrium) on the ovulation day, but type B (an echo of the endometrium similar to that of the surrounding uterine muscle layer) was predominant on the transfer day. From ovulation to the day of transfer in the overall population, there were no statistically significant differences in endometrial blood flow classification or subendometrial volume, but there was an increase in endometrial thickness (9.49±1.89 vs. 10.00±2.17 mm; P<0.001) and decreases in other indicators (P<0.05). The changes in the pregnant group were consistent with the direction of changes in the overall population, except for subendometrial volume (9.89±2.33 vs. 9.55±2.23 mL; P=0.017), whereas there were no significant differences in the nonpregnant group, except for the frequency of endometrial peristalsis (1.67±1.37 vs. 0.49±0.92 times/min; P<0.001). From ovulation to the day of transfer in the moderate-to-severe IUA population, there were significant increases in endometrial thickness (9.01±1.68 vs. 9.51±1.99 mm; P=0.002), vascularization index (VI; 1.92±2.58 vs. 1.99±3.39; P=0.019), and vascularization flow index (VFI; 0.65±1.18 vs. 0.72±1.46; P=0.010), whereas there were decreases in other indicators (P<0.05). From ovulation to the day of transfer in the mild IUA population, there was a significant increase in endometrial thickness (10.04±1.99 vs. 10.57±2.23 mm, P=0.011) and decreases in other indicators (P<0.05).
Conclusions: During natural cycles, in patients with a history of IUA, endometrial morphology mainly changed from type C to B, thickness increased, and the volume and frequency of peristalsis decreased. The blood supply of both the endometrium and subendometrium decreased significantly in the pregnant group. These findings provide a better understanding of the changes in ER in such patients, which is helpful for their pretransfer conversation.
Keywords: Endometrial receptivity (ER); intrauterine adhesion (IUA); ovulation day; transfer day; ultrasound evaluation.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-24-2034/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
The impact of intrauterine adhesions on endometrial receptivity in patients undergoing in vitro fertilization-embryo transfer.Front Endocrinol (Lausanne). 2025 Jan 21;15:1489839. doi: 10.3389/fendo.2024.1489839. eCollection 2024. Front Endocrinol (Lausanne). 2025. PMID: 39906037 Free PMC article.
-
Endometrial receptivity change: ultrasound evaluation on ovulation day and transplantation day during the natural frozen embryo transfer cycle.Front Endocrinol (Lausanne). 2023 Sep 26;14:1118044. doi: 10.3389/fendo.2023.1118044. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37822604 Free PMC article.
-
Detection of endometrial and subendometrial vasculature on the day of embryo transfer and prediction of pregnancy during fresh in vitro fertilization cycles.Taiwan J Obstet Gynecol. 2014 Sep;53(3):360-5. doi: 10.1016/j.tjog.2013.05.007. Taiwan J Obstet Gynecol. 2014. PMID: 25286791
-
Interceed combined with bone marrow mesenchymal stem cells improves endometrial receptivity of intrauterine adhesion.Regen Ther. 2024 Apr 25;27:445-454. doi: 10.1016/j.reth.2024.04.007. eCollection 2024 Dec. Regen Ther. 2024. PMID: 38706569 Free PMC article. Review.
-
Endometrial receptivity and intrauterine adhesive disease.Semin Reprod Med. 2014 Sep;32(5):392-401. doi: 10.1055/s-0034-1376358. Epub 2014 Jun 24. Semin Reprod Med. 2014. PMID: 24959821 Review.
References
-
- Katz Z, Ben-Arie A, Lurie S, Manor M, Insler V. Reproductive outcome following hysteroscopic adhesiolysis in Asherman's syndrome. Int J Fertil Menopausal Stud 1996;41:462-5. - PubMed
LinkOut - more resources
Full Text Sources