

Comparative analysis of different biopsy techniques for pancreatic lesions in diagnostic value, safety, and cost-effectiveness
- PMID: 40384725
- PMCID: PMC12084684
- DOI: 10.21037/qims-2024-2670
Comparative analysis of different biopsy techniques for pancreatic lesions in diagnostic value, safety, and cost-effectiveness
Abstract
Background: Pancreatic cancer is highly lethal and often diagnosed at an advanced stage, highlighting the need for early and accurate diagnosis. Although imaging plays a crucial role, definitive pathological confirmation requires biopsy. Percutaneous ultrasound-guided core needle biopsy (US-CNB), computed tomography-guided core needle biopsy (CT-CNB), and endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) are the three main biopsy techniques, each differing in diagnostic accuracy, safety, and cost-effectiveness. The aim of this study was to compare the diagnostic value, safety, and cost-effectiveness of these three biopsy techniques for suspiciously malignant pancreatic lesions.
Methods: We retrospectively evaluated patients with suspicious malignant pancreatic lesions who underwent US-CNB, CT-CNB, or EUS-FNA from January 2018 to January 2023. We compared technical success rates, sample adequacy, diagnostic accuracy, sensitivity, specificity, and complication rates of three groups. Additionally, we calculated the cost/effectiveness ratio (C/E) and incremental cost-effectiveness ratio (ICER) for each method.
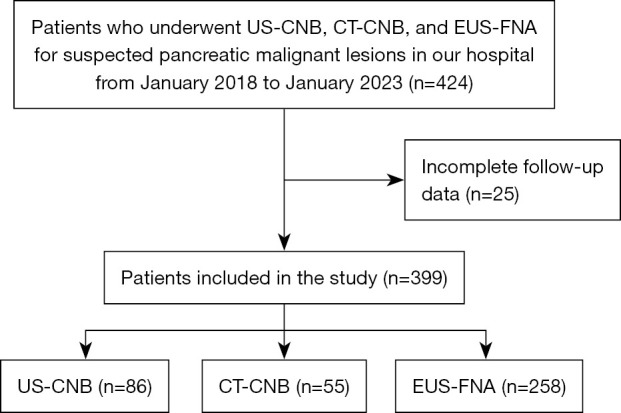
Results: A total of 399 patients were enrolled (US-CNB, n=86; CT-CNB, n=55; EUS-FNA, n=258), achieving 100% technical success. Sample adequacy satisfaction rates were 97.70% for US-CNB, 90.90% for CT-CNB, and 74.03% for EUS-FNA, with EUS-FNA significantly lower compared to the other two methods (P<0.001). Diagnostic accuracy was significantly higher for US-CNB (97.70%) and CT-CNB (90.90%) compared to EUS-FNA (69.80%) (P<0.001). Complication rates were 15.12% for US-CNB, 16.36% for CT-CNB, and 10.47% for EUS-FNA, with no significant differences (P=0.319). Compared to EUS-FNA, ICER for US-CNB was -14,367.7 yuan and for CT-CNB was -8,279.22 yuan per correct diagnosis, both below the willingness-to-pay threshold.
Conclusions: US-CNB and CT-CNB demonstrate superior diagnostic accuracy and specimen adequacy compared to EUS-FNA for suspected malignant pancreatic lesions. There are no significant differences in postoperative complication rates among three biopsy methods. In terms of cost-effectiveness, US-CNB and CT-CNB have lower costs and higher effectiveness than EUS-FNA, indicating greater economic efficiency.
Keywords: Pancreatic cancer; core needle biopsy (CNB); cost-effectiveness analysis; fine needle aspiration (FNA); ultrasound-guided.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-2024-2670/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Diagnostic Evaluation of Solid Pancreatic Lesions: Endoscopic Ultrasound-Guided Fine Needle Aspiration Versus Percutaneous Ultrasound-Guided Core Needle Biopsy.Cardiovasc Intervent Radiol. 2023 Nov;46(11):1596-1602. doi: 10.1007/s00270-023-03494-y. Epub 2023 Jul 18. Cardiovasc Intervent Radiol. 2023. PMID: 37464106
-
Comparison of Ultrasound-Guided Core Needle Biopsy and Endoscopic Ultrasound-Guided Fine-Needle Aspiration for Solid Pancreatic Lesions.J Ultrasound Med. 2015 Dec;34(12):2163-9. doi: 10.7863/ultra.14.11030. Epub 2015 Oct 21. J Ultrasound Med. 2015. PMID: 26491091
-
Percutaneous ultrasound and endoscopic ultrasound-guided biopsy of solid pancreatic lesions: An analysis of 1074 lesions.Hepatobiliary Pancreat Dis Int. 2023 Jun;22(3):302-309. doi: 10.1016/j.hbpd.2022.06.017. Epub 2022 Jul 4. Hepatobiliary Pancreat Dis Int. 2023. PMID: 35817668
-
Pretherapeutic evaluation of patients with upper gastrointestinal tract cancer using endoscopic and laparoscopic ultrasonography.Dan Med J. 2012 Dec;59(12):B4568. Dan Med J. 2012. PMID: 23290296 Review.
-
Meta-analysis of the diagnostic accuracy of ultrasound-guided fine-needle aspiration and core needle biopsy in diagnosing axillary lymph node metastasis.Br J Surg. 2018 Sep;105(10):1244-1253. doi: 10.1002/bjs.10920. Epub 2018 Jul 4. Br J Surg. 2018. PMID: 29972239
References
LinkOut - more resources
Full Text Sources