

Case Report: High efficacy of low-dose flecainide as an add-on therapy to a beta-blocker for treating a high burden of idiopathic ventricular arrhythmias in a juvenile athlete
- PMID: 40384969
- PMCID: PMC12081362
- DOI: 10.3389/fcvm.2025.1537078
Case Report: High efficacy of low-dose flecainide as an add-on therapy to a beta-blocker for treating a high burden of idiopathic ventricular arrhythmias in a juvenile athlete
Abstract
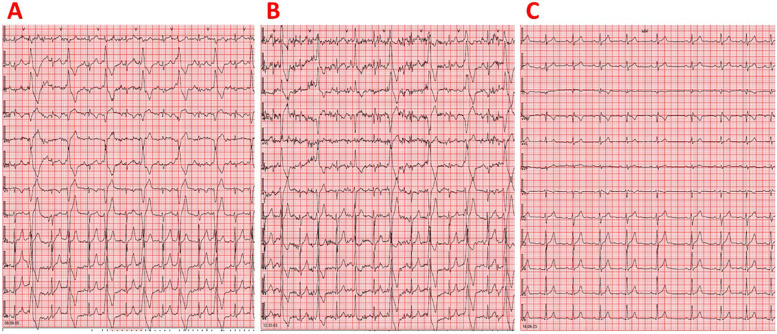
The detection of frequent premature ventricular contractions (PVCs) in an athlete represents one of the most important red flags during pre-participation screening. We report the case of a 6-year-old asymptomatic male athlete practicing basketball and sailing, who was examined for pre-participation screening. His resting electrocardiogram showed very frequent, isolated, monomorphic PVCs. The PVCs exhibited a left bundle branch block morphology with an inferior axis and R/S wave precordial transition in lead V3. The most likely origin of PVCs was considered the left ventricular outflow tract. Resting transthoracic echocardiography revealed reduced left ventricular systolic function, with an ejection fraction of 43%, indicating the possible existence of PVC-induced cardiomyopathy. We detected 43,149 isolated monomorphic PVCs (PVC burden: 40%) on 24-h ambulatory electrocardiographic monitoring. Initiation of treatment with atenolol 12.5 mg twice a day led to inadequate reduction of PVCs, with 29,452 isolated monomorphic PVCs (PVC burden: 29%) still observed on 24-h ambulatory electrocardiographic monitoring. After adding flecainide 25 mg twice daily to atenolol treatment, 24-h ambulatory electrocardiographic monitoring revealed complete resolution of ventricular arrhythmias, with no PVCs detected. Left ventricular systolic function recovered to normal. At 12 years of age, the athlete remained on combination therapy with atenolol and flecainide, continued participating in sports, and remained completely asymptomatic with normal cardiac examinations. The optimization of drug treatment was favored over catheter ablation since the athlete was a child and the probable origin of PVCs was the left ventricular outflow tract. This case report highlights that flecainide at a relatively low dose as an add-on therapy to a beta-blocker was highly effective and safe for treating high-burden PVCs originating from the ventricular outflow tract in a juvenile athlete.
Keywords: athlete; case report; flecainide; sports cardiology; ventricular arrhythmias.
© 2025 Christou, Letsas, Konstandi, Christou, Christou, Kyriakopoulos, Vidalakis, Tigas, Christodoulou and Kiortsis.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers at the time of submission. This had no impact on the peer review process and the final decision.
Figures

Similar articles
-
The R-S difference index: A new electrocardiographic method for differentiating idiopathic premature ventricular contractions originating from the left and right ventricular outflow tracts presenting a left bundle branch block pattern.Front Physiol. 2022 Sep 19;13:1002926. doi: 10.3389/fphys.2022.1002926. eCollection 2022. Front Physiol. 2022. PMID: 36200051 Free PMC article.
-
The role of pre-participation cardiac evaluation in the management of an athlete with premature ventricular contraction-induced cardiomyopathy: a case report.Eur Heart J Case Rep. 2022 May 16;6(5):ytac174. doi: 10.1093/ehjcr/ytac174. eCollection 2022 May. Eur Heart J Case Rep. 2022. PMID: 35582543 Free PMC article.
-
Effect of Flecainide in Idiopathic Premature Ventricular Contractions and the Induced Cardiomyopathy-UNIFLECA: A Single Arm, Non-Randomized Trial: Review of the Literature and Initial Results.J Pers Med. 2025 Mar 29;15(4):132. doi: 10.3390/jpm15040132. J Pers Med. 2025. PMID: 40278311 Free PMC article.
-
Are antiarrhythmic agents indicated in premature ventricular complex-induced cardiomyopathy and when?J Cardiovasc Electrophysiol. 2024 Mar;35(3):574-582. doi: 10.1111/jce.16055. Epub 2023 Sep 7. J Cardiovasc Electrophysiol. 2024. PMID: 37676022 Review.
-
Evaluation and Management of Premature Ventricular Complexes.Circulation. 2020 Apr 28;141(17):1404-1418. doi: 10.1161/CIRCULATIONAHA.119.042434. Epub 2020 Apr 27. Circulation. 2020. PMID: 32339046 Review.
References
Publication types
LinkOut - more resources
Full Text Sources