

Diffusion-weighted imaging and the Alberta Stroke Program Early CT Score (DWI-ASPECTS)-guided intra-arterial thrombectomy beyond 6 hours: feasibility, substantial efficacy, and acceptable safety
- PMID: 40385008
- PMCID: PMC12082544
- DOI: 10.62347/GLEJ7849
Diffusion-weighted imaging and the Alberta Stroke Program Early CT Score (DWI-ASPECTS)-guided intra-arterial thrombectomy beyond 6 hours: feasibility, substantial efficacy, and acceptable safety
Abstract
Objectives: To assess the safety and efficacy of intra-arterial thrombectomy for patients with acute ischemic stroke due to large vessel occlusion (LVO) treated beyond the traditional 6-hour window, using diffusion-weighted imaging and the Alberta Stroke Program Early CT Score (DWI-ASPECTS) for patient selection.
Methods: A retrospective study was conducted at Hebei General Hospital, involving 263 acute stroke patients treated between November 2022 and August 2024. Patients were categorized into two cohorts based on treatment timing: within 6 hours (n = 156) and beyond 6 hours (n = 107). Outcomes included the modified Rankin Scale (mRS), National Institutes of Health Stroke Scale (NIHSS), degree of vascular recanalization (modified Thrombolysis in Cerebral Infarction [mTICI] scale), coagulation parameters, and adverse event rates as safety measures.
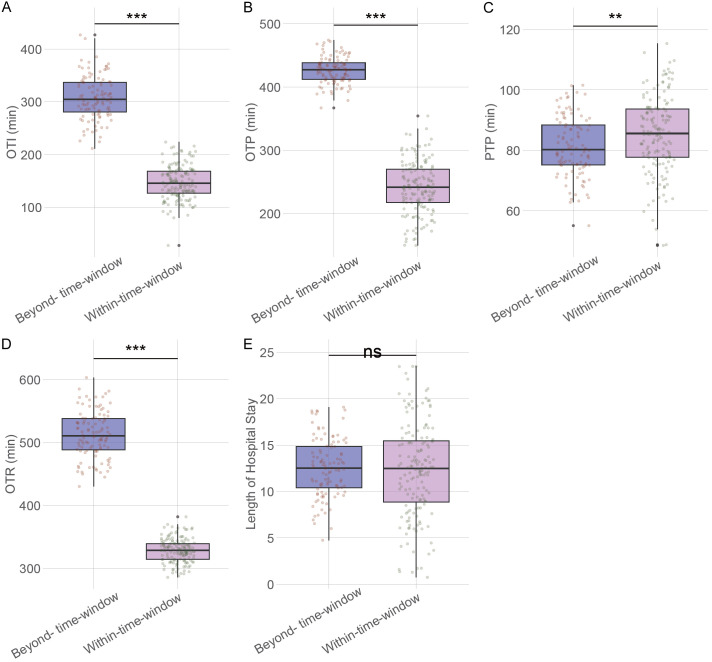
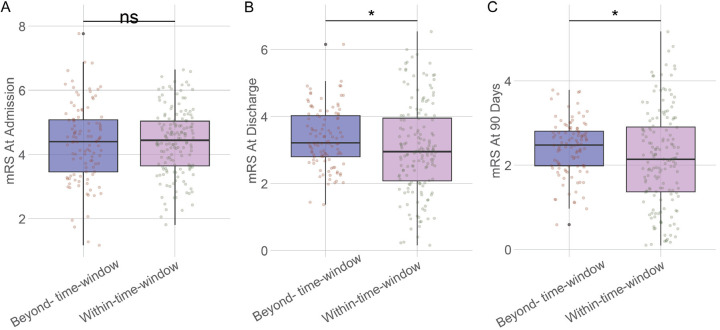
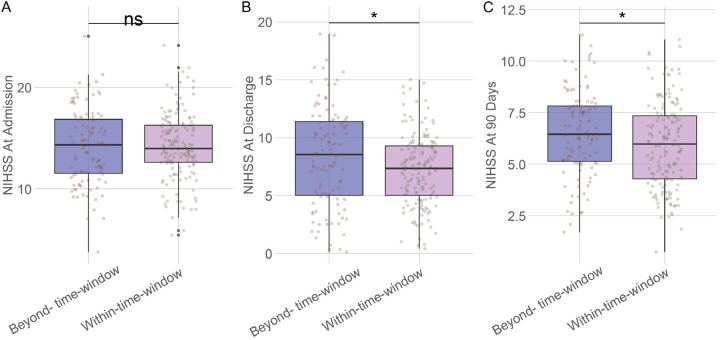
Results: Demographics and baseline conditions were comparable across groups. The beyond-6-hour group showed prolonged time from symptom onset to intervention, with slightly higher mRS and NIHSS scores at discharge and 90 days, indicating poorer functional and neurological outcomes (P < 0.05 for both). The beyond-6-hour group had a significantly lower vascular recanalization rate (mTICI ≥ 2b: 84.11%) compared to the within-6-hour group (93.59%, P = 0.013). However, the overall safety profile was similar, with no significant differences in adverse event rates.
Conclusion: Intra-arterial thrombectomy beyond the standard 6-hour window was feasible, showing substantial efficacy and an acceptable safety profile when guided by DWI-ASPECTS.
Keywords: Acute ischemic stroke; DWI-ASPECTS; large vessel occlusion; thrombectomy; treatment window; vascular recanalization.
AJTR Copyright © 2025.
Conflict of interest statement
None.
Figures
Similar articles
-
A direct aspiration first-pass technique vs stentriever thrombectomy in emergent large vessel intracranial occlusions.J Neurosurg. 2018 Feb;128(2):567-574. doi: 10.3171/2016.11.JNS161563. Epub 2017 Apr 14. J Neurosurg. 2018. PMID: 28409731
-
[Efficacy comparison of three vascular recanalization in patients with acute vertebrobasilar occlusion].Zhonghua Yi Xue Za Zhi. 2017 Apr 4;97(13):1001-1005. doi: 10.3760/cma.j.issn.0376-2491.2017.13.008. Zhonghua Yi Xue Za Zhi. 2017. PMID: 28395418 Chinese.
-
Clinical Impact and Predictors of Diffusion Weighted Imaging (DWI) Reversal in Stroke Patients with Diffusion Weighted Imaging Alberta Stroke Program Early CT Score 0-5 Treated by Thrombectomy : Diffusion Weighted Imaging Reversal in Large Volume Stroke.Clin Neuroradiol. 2022 Dec;32(4):939-950. doi: 10.1007/s00062-022-01156-z. Epub 2022 Apr 12. Clin Neuroradiol. 2022. PMID: 35412044
-
The Efficacy and Safety of Mechanical Thrombectomy in Posterior Circulation Large Vessel Occlusion as Compared to Anterior Circulation Large Vessel Occlusion: A Systematic Review.Cureus. 2023 Sep 24;15(9):e45861. doi: 10.7759/cureus.45861. eCollection 2023 Sep. Cureus. 2023. PMID: 37881373 Free PMC article. Review.
-
Mechanical thrombectomy in low Alberta stroke program early CT score (ASPECTS) in hyperacute stroke-a systematic review and meta-analysis.Br J Radiol. 2023 Dec;96(1152):20230084. doi: 10.1259/bjr.20230084. Epub 2023 Oct 24. Br J Radiol. 2023. PMID: 37873928 Free PMC article.
References
-
- Bhatia KD, Chowdhury S, Andrews I, Goetti R, Webster R, Troedson C, Dale RC, Muthusami P, Parra-Farinas C, Dlamini N, Moharir M, Miteff C, Miteff F, Worthington J, Tastula K, Ang T, Briest R, Pulcine E. Association between thrombectomy and functional outcomes in pediatric patients with acute ischemic stroke from large vessel occlusion. JAMA Neurol. 2023;80:910–918. - PMC - PubMed
-
- Costalat V, Lapergue B, Albucher JF, Labreuche J, Henon H, Gory B, Sibon I, Boulouis G, Cognard C, Nouri N, Richard S, Marnat G, Di Maria F, Annan M, Duhamel A, Cagnazzo F, Jovin T, Arquizan C LASTE Trial Investigators. Evaluation of acute mechanical revascularization in large stroke (ASPECTS ≤5) and large vessel occlusion within 7 h of last-seen-well: the LASTE multicenter, randomized, clinical trial protocol. Int J Stroke. 2024;19:114–119. - PubMed
-
- Farooqui M, Zaidat OO, Hassan AE, Quispe-Orozco D, Petersen N, Divani AA, Ribo M, Abraham M, Fifi J, Guerrero WR, Malik AM, Siegler JE, Nguyen TN, Sheth S, Yoo AJ, Linares G, Janjua N, Galecio-Castillo M, Tekle WG, Ringheanu VM, Oliver M, Dawod G, Kobsa J, Prasad A, Ikram A, Lin E, Below K, Zevallos CB, Gadea MO, Qureshi A, Dajles A, Matsoukas S, Rana A, Abdalkader M, Salazar-Marioni S, Soomro J, Gordon W, Vivanco-Suarez J, Turabova C, Mokin M, Yavagal DR, Jumaa MA, Ortega-Gutierrez S. Functional and safety outcomes of carotid artery stenting and mechanical thrombectomy for large vessel occlusion ischemic stroke with tandem lesions. JAMA Netw Open. 2023;6:e230736. - PMC - PubMed
-
- Saini V, Guada L, Yavagal DR. Global epidemiology of stroke and access to acute ischemic stroke interventions. Neurology. 2021;97(Suppl 2):S6–S16. - PubMed
LinkOut - more resources
Full Text Sources