

Factors influencing the development of heart failure after PCI in patients with acute coronary syndrome: a meta-analysis
- PMID: 40385038
- PMCID: PMC12082520
- DOI: 10.62347/FPXH3010
Factors influencing the development of heart failure after PCI in patients with acute coronary syndrome: a meta-analysis
Abstract
Objective: To systematically analyze the factors associated with heart failure (HF) development after percutaneous coronary intervention (PCI) in patients with acute coronary syndrome (ACS).
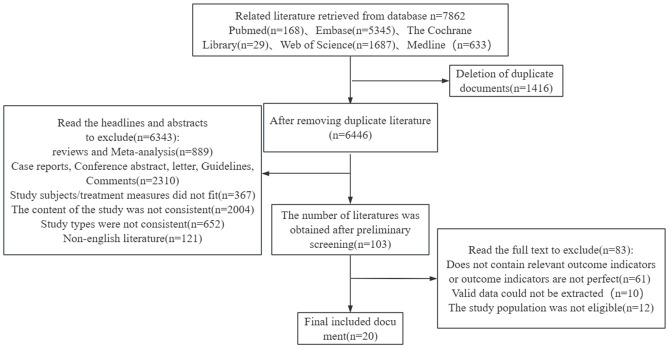
Methods: Relevant literature on risk factors for HF following PCI in ACS patients were retrieved from PubMed, Embase, The Cochrane Library, Web of Science, and Medline buildup to September 2024. Two independent investigators conducted literature screening, quality assessment, and data extraction based on inclusion and exclusion criteria. Meta-analysis was performed using Stata 12.0 software.
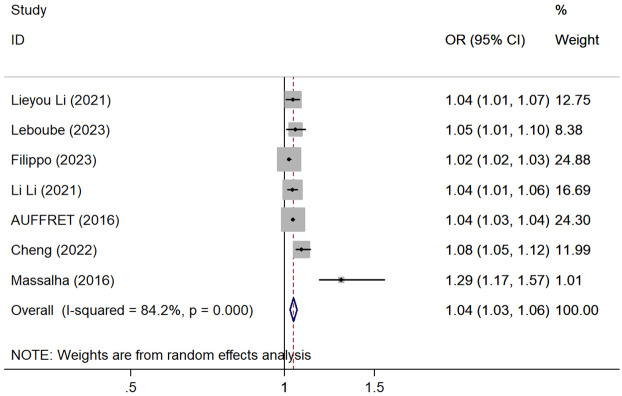
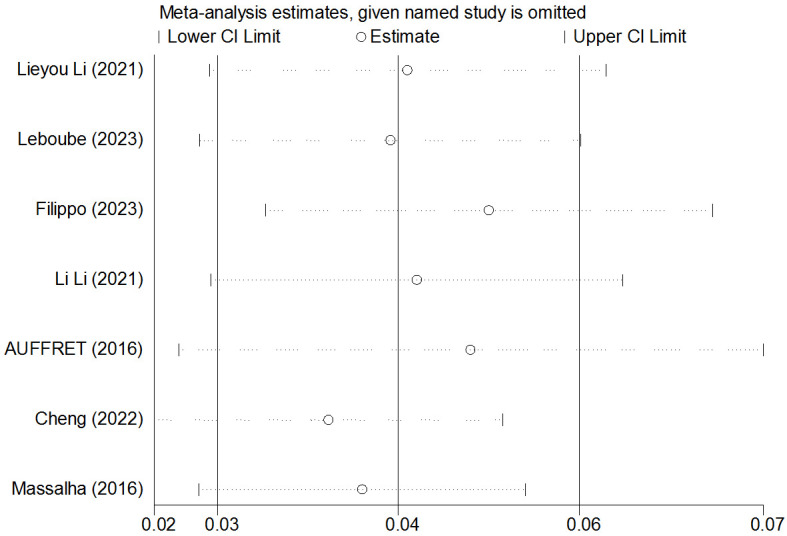
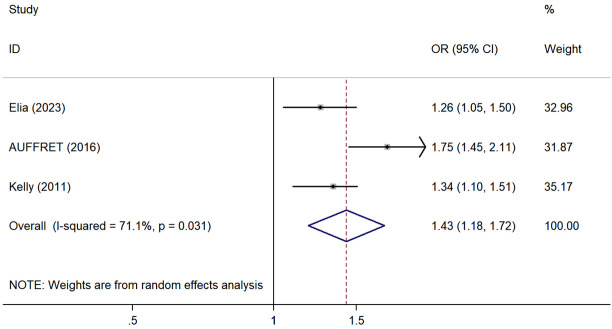
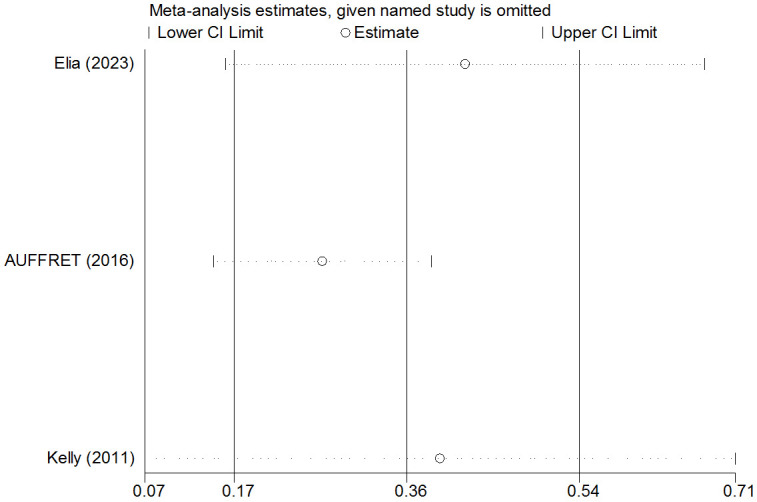
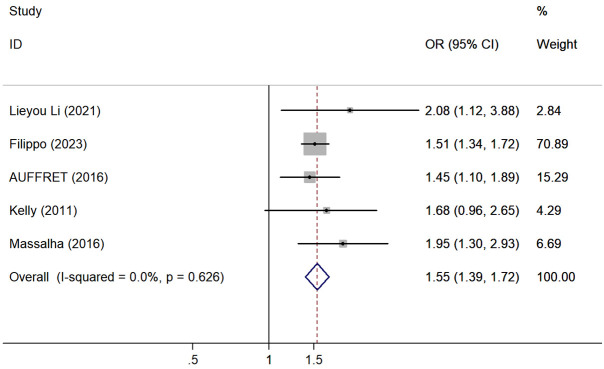
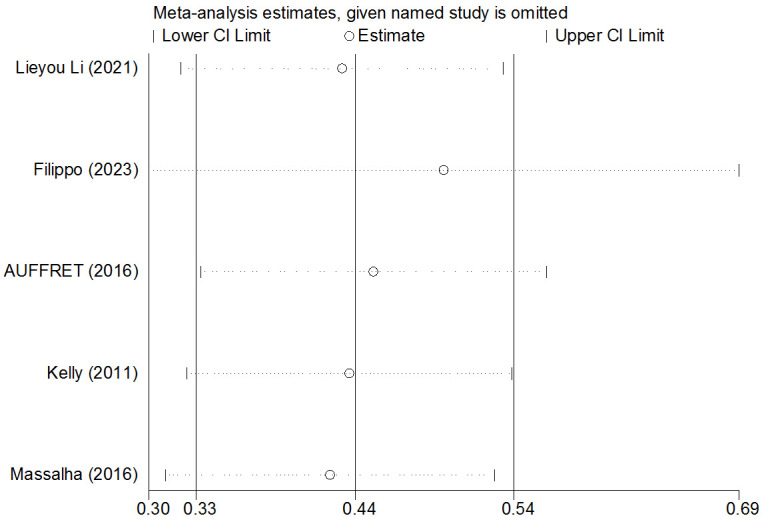
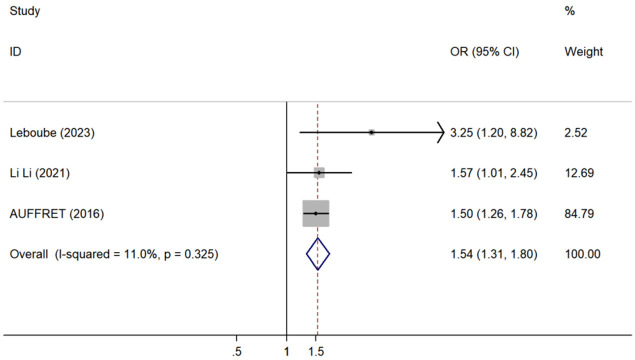
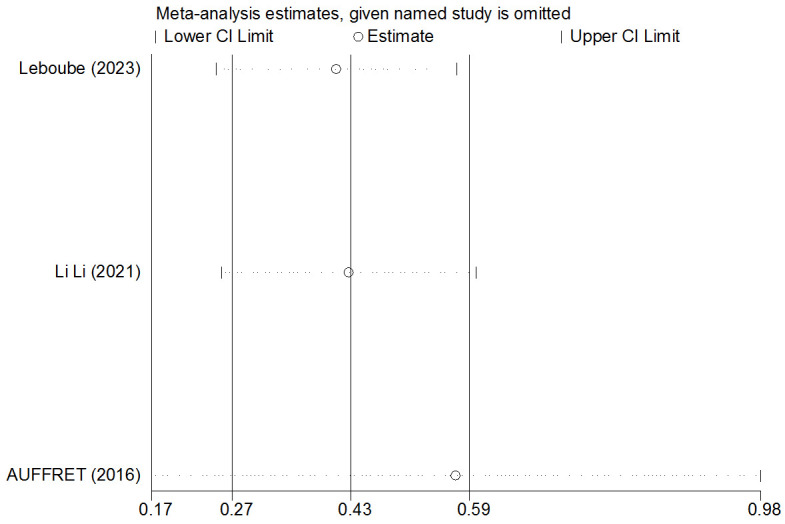
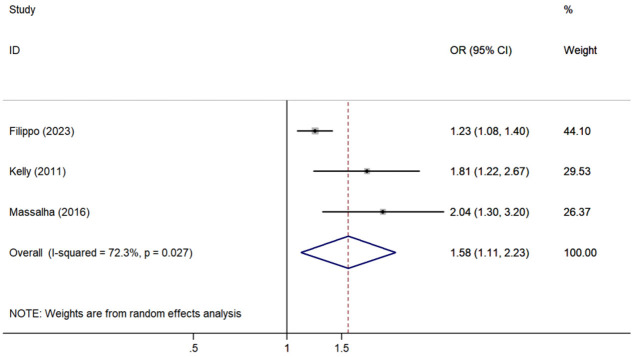
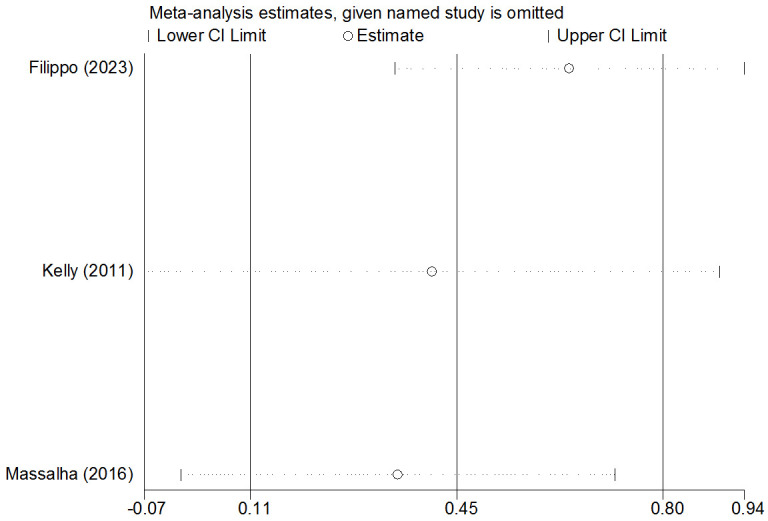
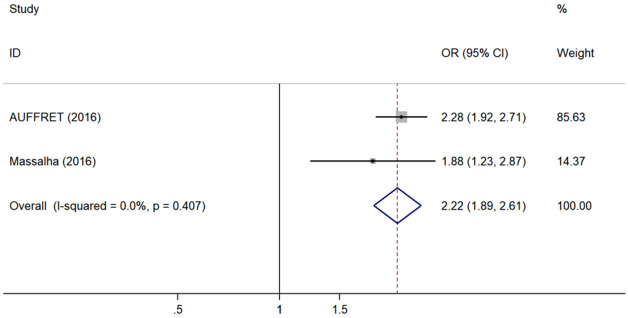
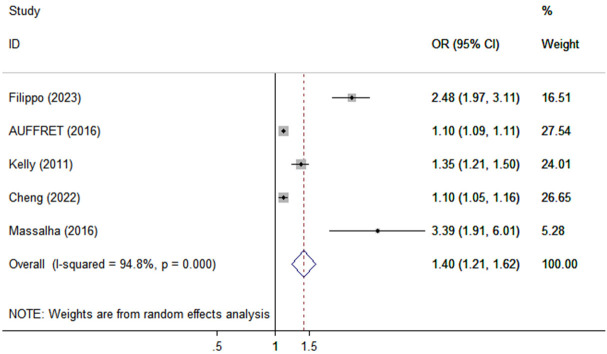
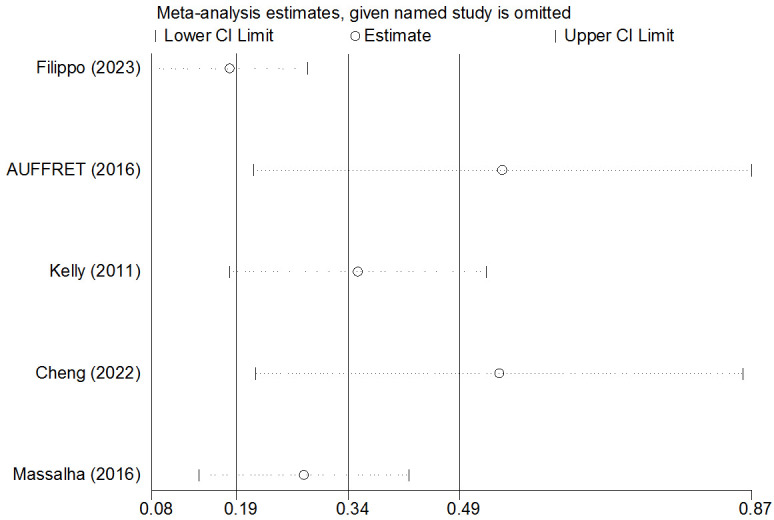
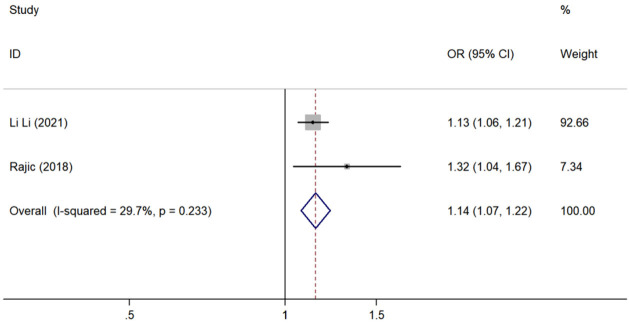
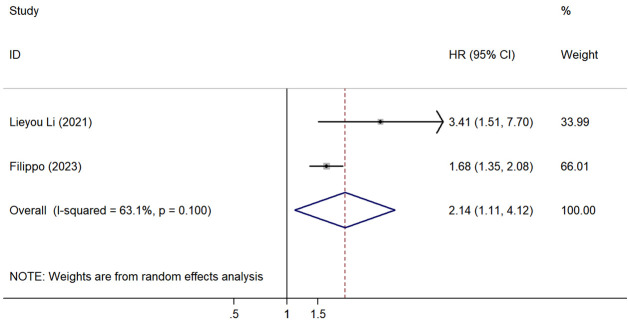
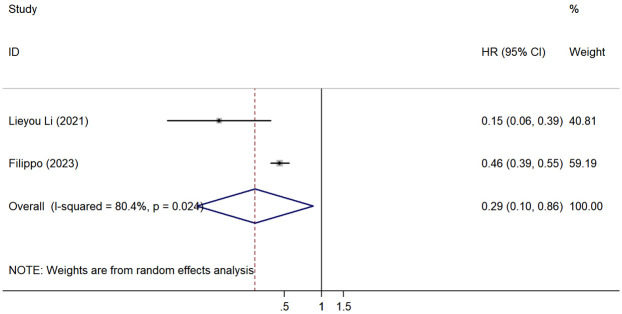
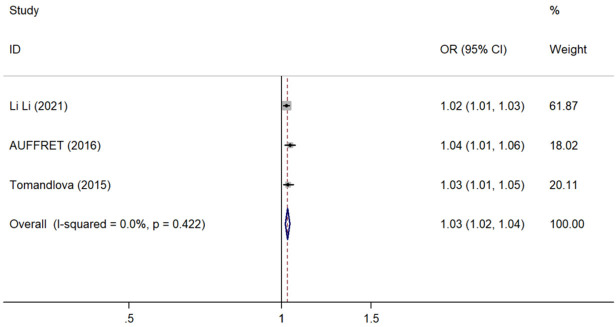
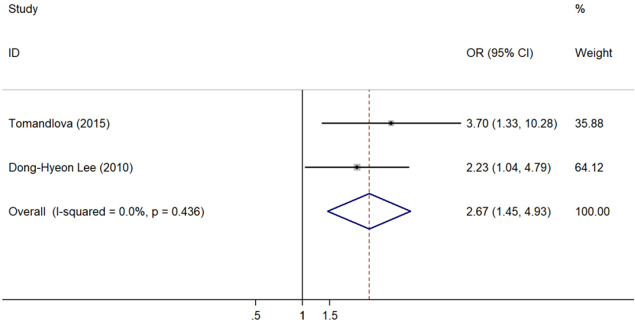
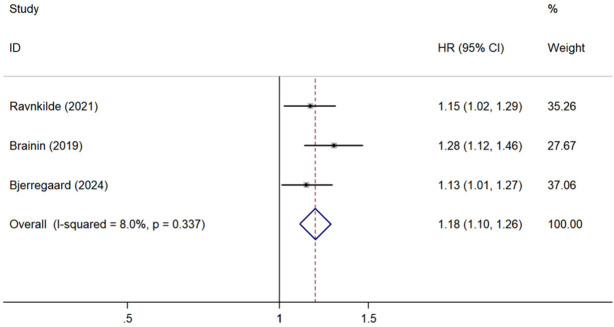
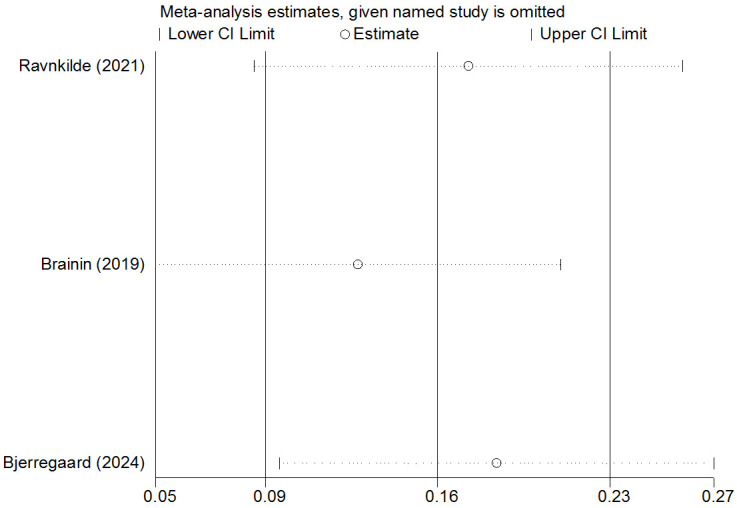
Results: A total of 20 papers were included, comprising 45,578 patients of whom 4,345 ACS patients developed HF after PCI. Meta-analysis identified several predictors of post-PCI HF in ACS patients, including advanced age [odds ratio (OR) =1.04, 95% confidence intervals (CI): 1.03-1.06], female gender (OR=1.43, 95% CI: 1.18-1.72), history of hypertension (OR=1.54, 95% CI: 1.31-1.80), history of diabetes mellitus (OR=1.55, 95% CI: 1.39-1.72), previous myocardial infarction (OR=1.58, 95% CI: 1.11-2.23), anterior wall myocardial infarction (OR=2.22, 95% CI: 1.89-2.61), reduced left ventricular ejection fraction (LVEF) (OR=1.40, 95% CI: 1.21-1.62), elevated white blood cell count (OR=1.14, 95% CI: 1.07-1.22), atrial fibrillation [hazard ratio (HR) =2.14, 95% CI: 1.11-4.12], increased heart rate (OR=1.03, 95% CI: 1.02-1.04), elevated Pentraxin-3 (PTX3) levels (OR=2.67, 95% CI: 1.45-4.93), and decreased myocardial contractility (HR=1.18, 95% CI: 1.10-1.26). Notably, complete revascularization (HR=0.29, 95% CI: 0.10-0.86) was identified as a protective factor. Sensitivity analysis confirmed the robustness of these findings.
Conclusions: Advanced age, female gender, history of hypertension and diabetes, previous myocardial infarction, anterior wall myocardial infarction, decreased LVEF at admission, increased white blood cell count, atrial fibrillation at admission, increased heart rate, elevated PTX3 levels, and impaired myocardial contractility were risk factors for HF development after PCI in ACS patients. Conversely, complete revascularization was associated with a lower risk of post-PCI HF.
Keywords: Acute coronary syndrome; PCI; heart failure; influencing factors; meta-analysis.
AJTR Copyright © 2025.
Conflict of interest statement
None.
Figures
Similar articles
-
Improved heart function and cardiac remodelling following sacubitril/valsartan in acute coronary syndrome with HF.ESC Heart Fail. 2024 Apr;11(2):937-949. doi: 10.1002/ehf2.14646. Epub 2024 Jan 15. ESC Heart Fail. 2024. PMID: 38224955 Free PMC article.
-
IncidenCe and predictOrs of heaRt fAiLure after acute coronarY Syndrome: The CORALYS registry.Int J Cardiol. 2023 Jan 1;370:35-42. doi: 10.1016/j.ijcard.2022.10.146. Epub 2022 Oct 25. Int J Cardiol. 2023. PMID: 36306949
-
Effects of Percutaneous Coronary Intervention and Coronary Artery Bypass Grafting on Clinical Outcomes in Patients with Reduced Ejection Fraction Heart Failure and Coronary Heart Disease: A Meta-Analysis.Heart Surg Forum. 2023 Feb 10;26(1):E062-E073. doi: 10.1532/hsf.5169. Heart Surg Forum. 2023. PMID: 36856505
-
Clinical Efficacy and Safety of Early Intravenous Administration of Beta-Blockers in Patients Suffering from Acute ST-Segment Elevation Myocardial Infarction Without Heart Failure Undergoing Primary Percutaneous Coronary Intervention: A Study-Level Meta-Analysis of Randomized Clinical Trials.Cardiovasc Drugs Ther. 2024 Aug;38(4):833-846. doi: 10.1007/s10557-023-07448-x. Epub 2023 Apr 1. Cardiovasc Drugs Ther. 2024. PMID: 37002468 Free PMC article.
-
Prevalence and Predictors of Contrast-Induced Nephropathy (CIN) in Patients with ST-Segment Elevation Myocardial Infarction (STEMI) Undergoing Percutaneous Coronary Intervention (PCI): A Meta-Analysis.J Interv Cardiol. 2019 Aug 25;2019:2750173. doi: 10.1155/2019/2750173. eCollection 2019. J Interv Cardiol. 2019. PMID: 31772520 Free PMC article. Review.
References
-
- Atwood J. Management of acute coronary syndrome. Emerg Med Clin North Am. 2022;40:693–706. - PubMed
-
- Charles-Schoeman C, Buch MH, Dougados M, Bhatt DL, Giles JT, Ytterberg SR, Koch GG, Vranic I, Wu J, Wang C, Kwok K, Menon S, Rivas JL, Yndestad A, Connell CA, Szekanecz Z. Risk of major adverse cardiovascular events with tofacitinib versus tumour necrosis factor inhibitors in patients with rheumatoid arthritis with or without a history of atherosclerotic cardiovascular disease: a post hoc analysis from ORAL Surveillance. Ann Rheum Dis. 2023;82:119–129. - PMC - PubMed
-
- Ren XY, Li YF, Liu HQ, Lin H, Lin Q, Wu Y, Wan J, Lu JJ, Liu J, Cui XY. Anti-inflammatory therapy progress in major adverse cardiac events after PCI: Chinese and western medicine. Chin J Integr Med. 2023;29:655–664. - PubMed
-
- Liu S, Guo X, Wu D, Zhang AL, Xue C, Wen Z. Construction of clinical evidence grading system of TCM intervention based on evidence-based medicine principles. Chinese Journal of Integrated Medicine. 2023;43:1885–1889.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous