

Factors influencing the diagnostic accuracy of lung cancer using endobronchial ultrasound-guided transbronchial needle aspiration
- PMID: 40385055
- PMCID: PMC12082559
- DOI: 10.62347/UIGU6267
Factors influencing the diagnostic accuracy of lung cancer using endobronchial ultrasound-guided transbronchial needle aspiration
Abstract
Objectives: Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a key diagnostic modality for lung cancer, yet its accuracy varies based on several factors. This study aims to identify factors influencing the diagnostic accuracy of EBUS-TBNA for lung cancer detection.
Methods: A retrospective case-control study was conducted on lung cancer patients diagnosed at Gaozhou People's Hospital from October 2021 to September 2023. Patients with lung cancer confirmed by EBUS-TBNA, bronchoscopy with direct biopsy, or surgical intervention were re-evaluated using EBUS-TBNA. Based on diagnostic accuracy, they were classified into an accurate group (n = 204) and an inaccurate group (n = 41). An external validation cohort included 58 lung cancer patients. Data collection encompassed patient demographics and EBUS-TBNA findings. Logistic regression and receiver operating characteristic (ROC) curve analyses were performed to determine factors influencing detection accuracy. A generalized linear model incorporating independent influencing factors was developed to estimate the likelihood of inaccurate EBUS-TBNA detection of lung cancer.
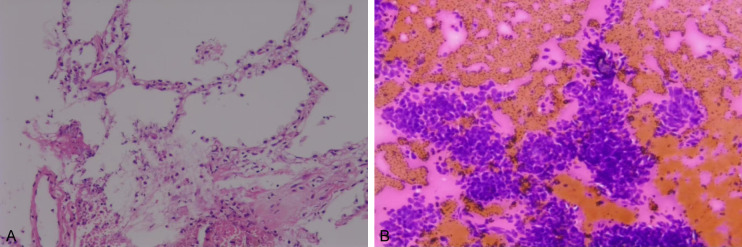
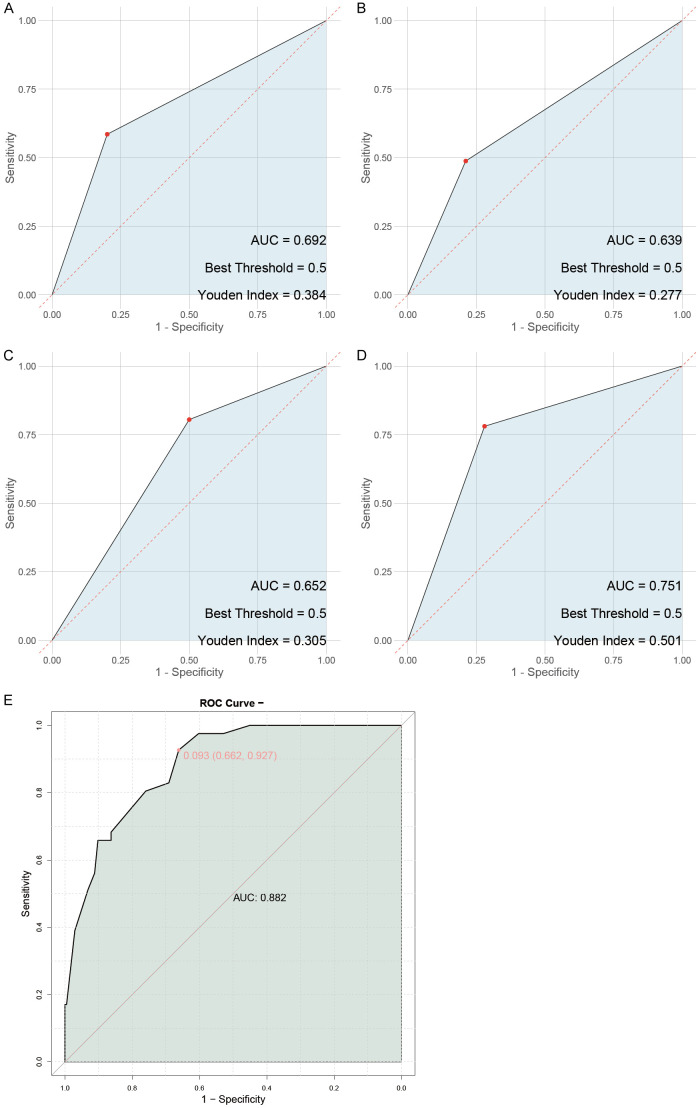
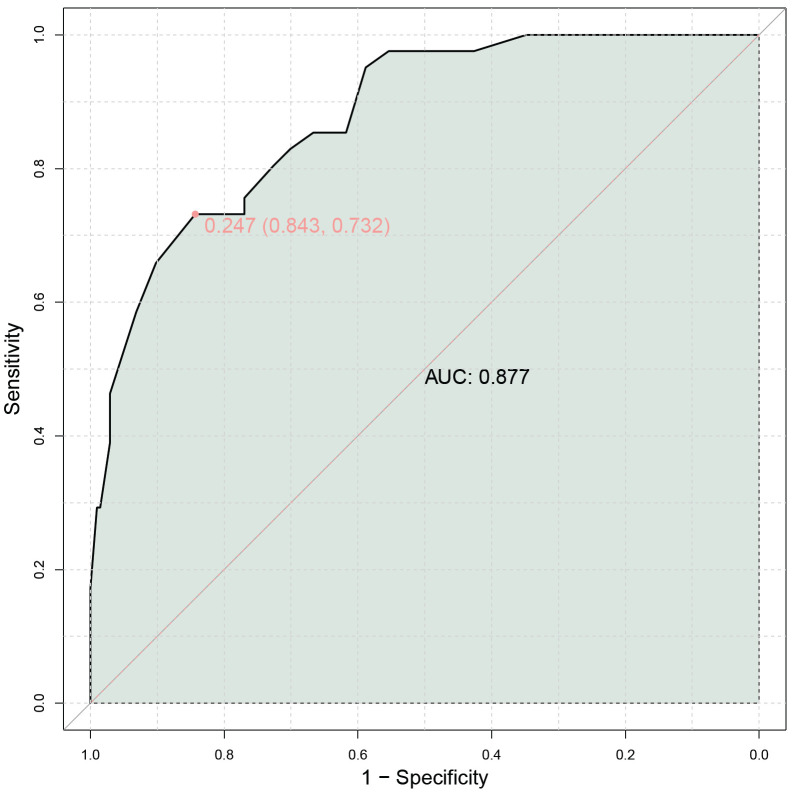
Results: Smoking history [dds ratio (OR), 7.948; P < 0.001] and a diagnosis of small cell lung cancer (OR, 3.996; P = 0.007) were significantly associated with an increased risk of inaccurate detection. In contrast, a lesion diameter of ≥ 3 cm (OR, 0.343; P = 0.026) and linear filamentous changes in aspirate samples (OR, 0.106; P < 0.001) were strongly correlated with accurate detection. Larger lesion size and specific sample characteristics were also significant predictors in the external validation cohort (P < 0.05). Multivariate logistic regression confirmed these factors as independent predictors of diagnostic accuracy. The predictive model demonstrated robust performance [area under the curve (AUC) = 0.882], with external validation yielding a comparable AUC of 0.877.
Conclusion: Smoking history, pathologic subtype, lesion size and aspirate sample characteristics significantly affected the diagnostic accuracy of EBUS-TBNA in lung cancer detection. These insights underscore the importance of considering these factors in clinical practice to optimize EBUS-TBNA's diagnostic performance.
Keywords: Lung cancer; diagnostic accuracy; endobronchial ultrasound-guided transbronchial needle aspiration; lesion size; predictive model; smoking history.
AJTR Copyright © 2025.
Conflict of interest statement
None.
Figures
Similar articles
-
Learning curves and association of pathologist's performance with the diagnostic accuracy of linear endobronchial ultrasound transbronchial needle aspiration (EBUS-TBNA): a cohort study in a tertiary care reference centre.BMJ Open. 2022 Oct 19;12(10):e051257. doi: 10.1136/bmjopen-2021-051257. BMJ Open. 2022. PMID: 36261243 Free PMC article.
-
Comparative yield of EBUS-TBNA with EBUS-IFBTLP for diagnosis of mediastinal lymphadenopathy.Ther Adv Respir Dis. 2024 Jan-Dec;18:17534666241282217. doi: 10.1177/17534666241282217. Ther Adv Respir Dis. 2024. PMID: 39340275 Free PMC article.
-
A retrospective study of endobronchial ultrasound transbronchial needle aspiration versus conventional transbronchial needle aspiration in diagnosis/staging of hilar/mediastinal lymph node in lung cancer: Which role in clinical practice?Monaldi Arch Chest Dis. 2019 Apr 17;89(1). doi: 10.4081/monaldi.2019.1010. Monaldi Arch Chest Dis. 2019. PMID: 30996353
-
Comparing diagnostic sensitivity of different needle sizes for lymph nodes suspected of lung cancer in endobronchial ultrasound transbronchial needle aspiration: Systematic review and meta-analysis.Clin Respir J. 2021 Dec;15(12):1328-1336. doi: 10.1111/crj.13436. Epub 2021 Aug 31. Clin Respir J. 2021. PMID: 34402194
-
Comparison between Endobronchial Ultrasound-Guided Transbronchial Node Biopsy and Transbronchial Needle Aspiration: A Meta-Analysis.Respiration. 2024;103(12):752-764. doi: 10.1159/000540859. Epub 2024 Aug 13. Respiration. 2024. PMID: 39137742
References
-
- Chen M, Liu J, Wang D, Wang H, Liang J, Li Z. Analysis of fever following bronchoscopy and endobronchial ultrasound-guided transbronchial needle aspiration. Altern Ther Health Med. 2024;30:254–259. - PubMed
-
- Kajita Y, Teranishi S, Sawazumi T, Watanabe H, Nagaoka S, Tanaka A, Suzukawa Y, Motobayashi Y, Hirose T, Maeda C, Seki K, Tashiro K, Kobayashi N, Yamamoto M, Kudo M, Inayama Y, Kaneko T. Comparison of the slow-pull and aspiration methods of endobronchial ultrasound-guided transbronchial needle aspiration for next-generation sequencing-compatible tissue collection in non-small cell lung cancer. Cancer Med. 2023;12:19512–19522. - PMC - PubMed
-
- Chung K, Bentel J, Laycock A. Accuracy of endobronchial ultrasound-guided transbronchial needle aspiration for staging of non-small cell lung cancer. Diagn Cytopathol. 2024;52:254–263. - PubMed
-
- Vuorisalo A, Huhtala H, Paavonen T, Kholová I. Insufficient endobronchial ultrasound-guided transbronchial needle aspiration specimens. When and why? The analysis of criteria and reasons behind the insufficient specimens. Diagn Cytopathol. 2024;52:271–287. - PubMed
-
- Lindquist KE, Cortas G, Hashemi Y, Rajabian N, Ehinger M. Endobronchial ultrasound-guided transbronchial fine needle aspiration of mediastinal lymphadenopathy: diagnostic performance and clinical implications of the World Health Organization reporting system. Diagn Cytopathol. 2024;52:524–532. - PubMed
LinkOut - more resources
Full Text Sources