

Unveiling the role of stress hyperglycemia in predicting mortality for critically ill hemorrhagic stroke patients: insights from MIMIC-IV
- PMID: 40385356
- PMCID: PMC12081252
- DOI: 10.3389/fendo.2025.1558352
Unveiling the role of stress hyperglycemia in predicting mortality for critically ill hemorrhagic stroke patients: insights from MIMIC-IV
Abstract
Background: Hemorrhagic stroke (HS), including intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH), is associated with high mortality and morbidity. Stress hyperglycemia ratio (SHR), reflecting acute glycemic responses relative to baseline glucose levels, has been linked to poor outcomes in critical illnesses. However, research on its prognostic significance in HS patients admitted to the intensive care unit (ICU) is limited. This study aims to assess the association between SHR and all-cause mortality (ACM) in critically ill HS patients.
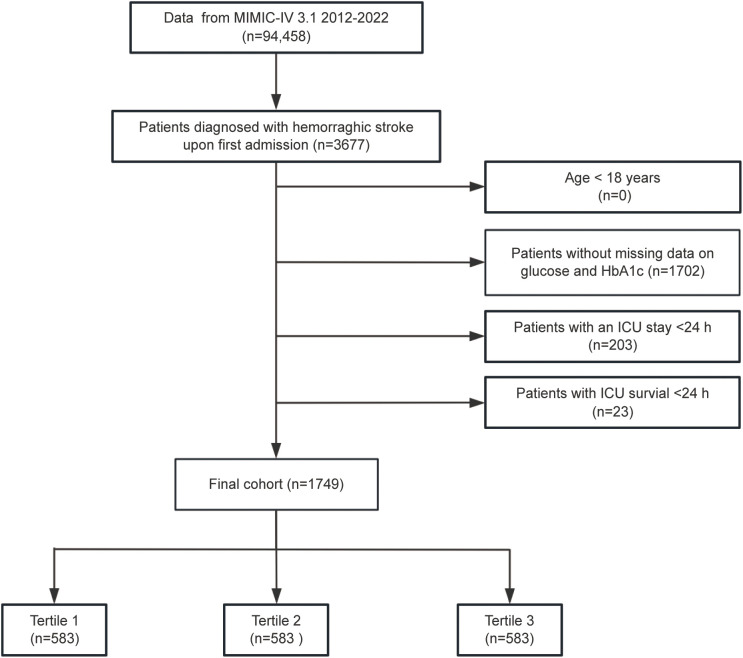
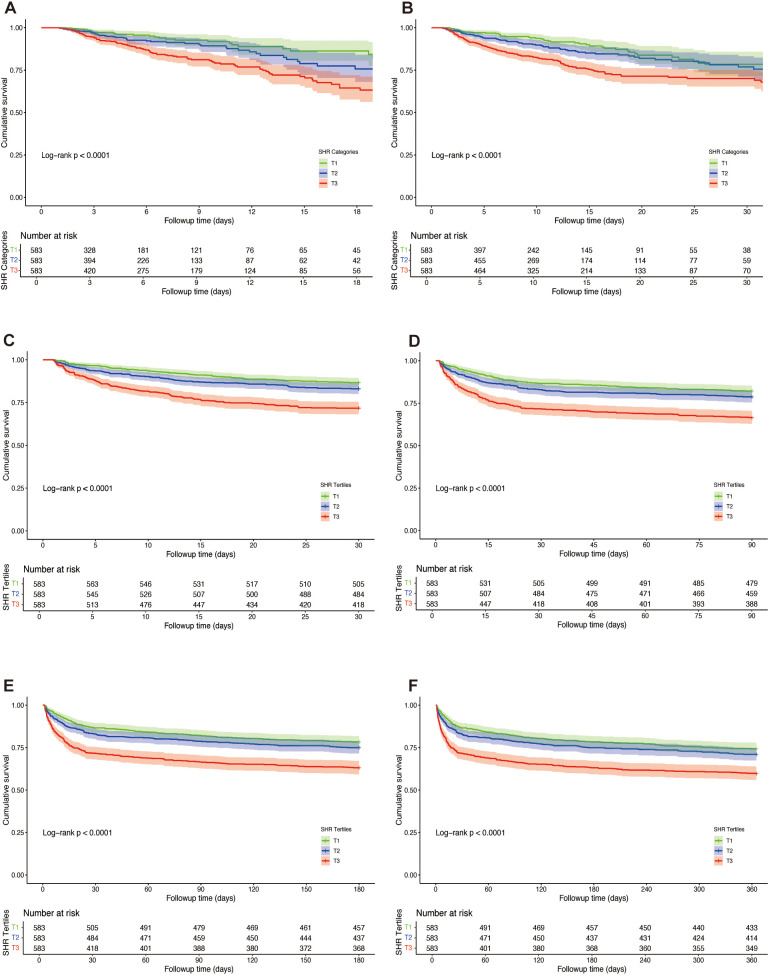
Methods: Patients diagnosed with HS were extracted from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database using ICD-9/10 codes. SHR was calculated as [admission glucose (mg/dL)/(28.7 × HbA1c (%) - 46.7)]. Patients were stratified into tertiles. Primary outcomes were ICU, in-hospital, 30-day, 90-day, 180-day, and 1-year mortality. Cox regression and restricted cubic splines (RCS) evaluated the dose-response relationship between SHR and ACM. Kaplan-Meier (K-M) analysis assessed survival across tertiles, with subgroup analysis and interaction tests for effect modification.
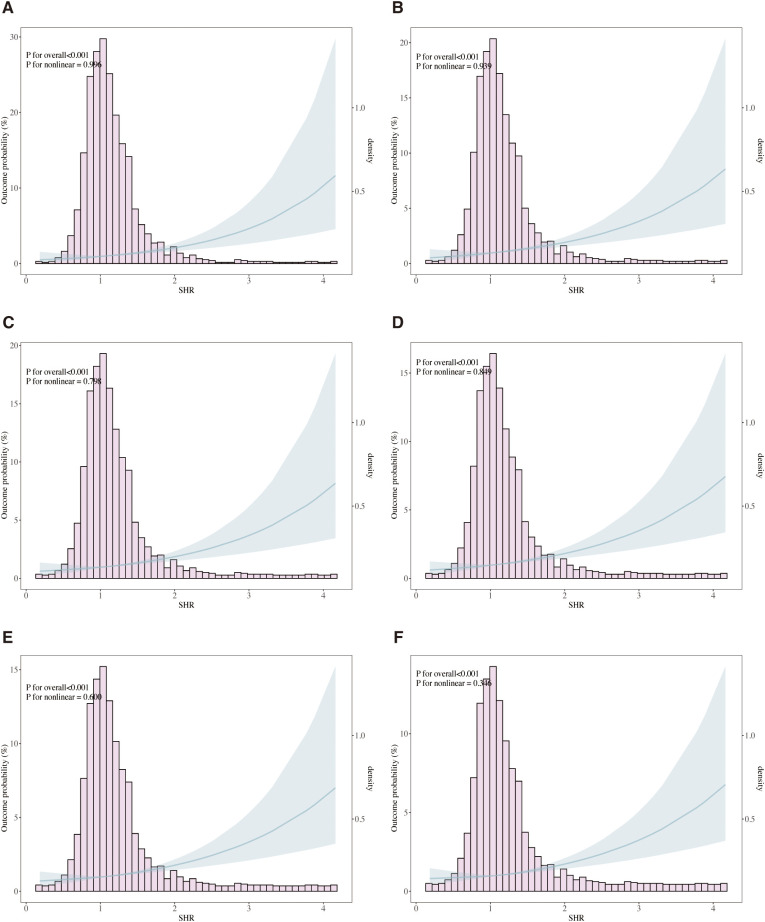
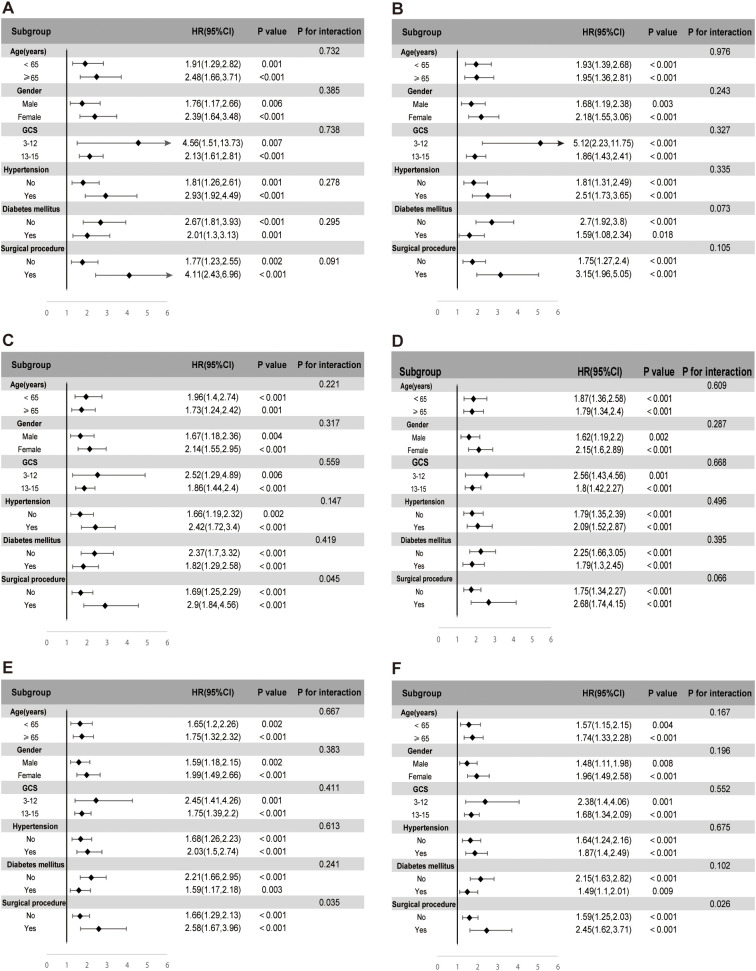
Results: The study included 1,749 patients, with a median age of 68 years (IQR: 57-79), and 53.2% were male. The observed mortality rates were 10.6% in the ICU, 15.2% in-hospital, 19.6% at 30 days, 24.2% at 90 days, 27.8% at 180 days, and 31.7% at 1 year. Multivariate Cox regression analysis indicated that elevated SHR was independently associated with increased ACM at 30 days (adjusted hazard ratio [aHR]: 1.41; 95% confidence interval [CI]: 1.10-1.81; P = 0.006), 90 days (aHR: 1.33; 95% CI: 1.08-1.65; P = 0.008), and 1 year (aHR: 1.27; 95% CI: 1.05-1.54; P = 0.014). RCS analysis demonstrated a linear association between SHR and ACM, with no evidence of non-linearity. Subgroup analysis revealed consistent associations across various patient characteristics.
Conclusion: SHR is significantly associated with ACM in critically ill patients with HS, supporting its potential role as a prognostic marker for risk stratification and guiding clinical management. Incorporating SHR into routine risk assessment may facilitate early identification of high-risk patients, enabling timely interventions and improved outcomes.
Keywords: MIMIC-IV database; all-cause mortality; hemorrhagic stroke; prognosis; stress hyperglycemia ratio.
Copyright © 2025 Yue, Li, Sun, Wang, Li and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical