

Integration of minimally invasive techniques and interventional therapy: application of percutaneous nephrolithotomy in patients with upper urinary tract stones and an analysis of risk factors for postoperative bleeding
- PMID: 40385576
- PMCID: PMC12081443
- DOI: 10.3389/fmed.2025.1556224
Integration of minimally invasive techniques and interventional therapy: application of percutaneous nephrolithotomy in patients with upper urinary tract stones and an analysis of risk factors for postoperative bleeding
Abstract
Background: Percutaneous nephrolithotomy is one of the preferred treatment options for upper urinary tract stones. However, postoperative bleeding remains a clinical challenge. It is crucial to identify the effectiveness of this procedure and understand the risk factors causing postoperative bleeding.
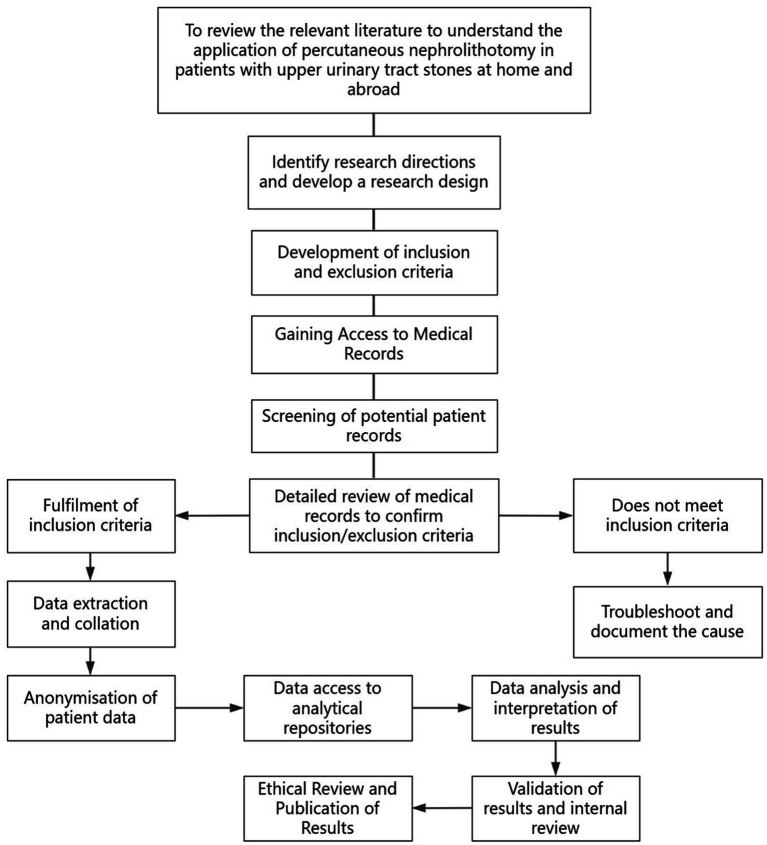
Methods: A total of 383 patients with upper urinary tract stones included in our hospital from March 2020 to February 2024 were retrospectively selected and divided into 2 groups as per different treatments. A total of 204 patients who underwent guidewire-assisted percutaneous nephrolithotomy were included in the guidewire-assisted group, while the other 179 patients who underwent conventional percutaneous nephrolithotomy were enrolled in the conventional group for a comparison of treatment effects. Then, single-factor and multifactorial logistic regressions in accordance with the postoperative bleeding situation were conducted to analyze the risk factors of postoperative bleeding in patients with upper urinary tract stones.
Results: The results showed that the guidewire-assisted percutaneous nephrolithotomy group had a higher stone removal rate compared to the conventional group, with lower rates of complications, operation time, gastrointestinal recovery time, hospital stay, postoperative bleeding, and hemoglobin drop (p < 0.05). There was no significant difference in stone recurrence rate (p > 0.05). Among the 383 patients studied, 39 experienced severe bleeding (≥400 mL), while 344 had minor bleeding (<400 mL). Factors significantly associated with postoperative bleeding included the history of diabetes, preoperative blood creatinine, surgical method, staghorn calculi, hydronephrosis, and renal parenchymal thickness difference (p < 0.05). However, collinearity was noted between diabetes history and staghorn calculi. After adjustment of these variables, preoperative blood creatinine, surgical modality, hydronephrosis, and renal parenchymal thickness emerged as key predictors of postoperative bleeding.
Conclusion: Compared to conventional percutaneous nephrolithotomy, guidewire-assisted percutaneous nephrolithotomy could improve the stone removal rate of patients with upper urinary tract stones and reduce the occurrence of complications, while some patients were still prone to the postoperative bleeding phenomenon, which might be closely related to the preoperative Scr, surgical methods, hydronephrosis, and renal parenchymal thickness. The mentioned phenomenon needed clinical attention and corresponding measures to intervene as soon as possible to reduce the bleeding in the postoperative period.
Keywords: guidewire-assisted; percutaneous nephrolithotomy; postoperative bleeding; risk factors; upper urinary tract stone.
Copyright © 2025 Sun and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources