

Brachial plexus injuries in the contact athlete: a narrative review
- PMID: 40385690
- PMCID: PMC12082188
- DOI: 10.21037/aoj-24-67
Brachial plexus injuries in the contact athlete: a narrative review
Abstract
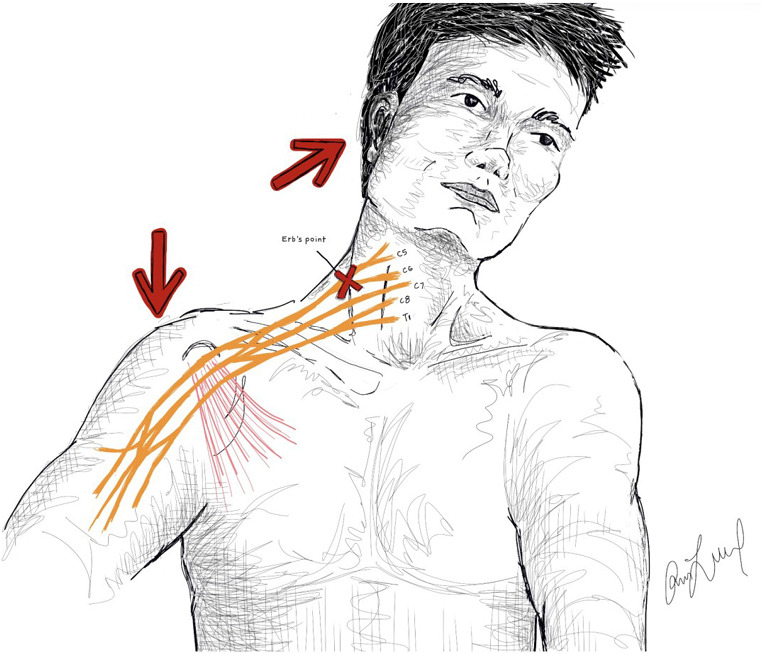
Background and objective: Brachial plexus injuries (BPIs) are a rare but potentially devastating injury among contact athletes. More common injuries, such as "burners" or "stingers", indicate a temporary and less severe insult to either the nerve roots or plexus. The aim of this review is to discuss this spectrum of injuries in their epidemiology, mechanism in contact sports, diagnosis, and treatment.
Methods: This literature review utilized key terms to search manuscripts available in English from inception to October 2024 within three research databases.
Key content and findings: BPIs among contact athletes occur on a spectrum from neuropraxia to neurotmesis. Neuropraxia is very common among contact athletes with approximately a 49-65% incidence among career football players with the most common mechanism being a traction injury. Most of these resolve within minutes to hours. Axonotmesis and neurotmesis can be far more severe injuries and require further investigation if not resolved by 2-3 weeks. The majority of athletes who suffer neuropraxic injuries will return to sport with minimal to no time missed, however, more severe injuries portend variable outcomes.
Conclusions: BPIs are common among contact athletes and involve a spectrum of nerve damage, of which most are self-limiting. However, further evaluation is warranted when symptoms last beyond 2-3 weeks. Future studies should focus on treatment algorithms and long-term outcomes, including return to sport.
Keywords: Brachial plexus injury (BPI); burner; contact athletes; sports; stinger.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://aoj.amegroups.com/article/view/10.21037/aoj-24-67/coif). The series “Care of the Contact Athlete’s Shoulder” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures

References
-
- Tosti R, Rossy W, Sanchez A, et al. Burners, stingers, and other brachial plexus injuries in the contact athlete. Oper Tech Sports Med 2016;24:273-7. 10.1053/j.otsm.2016.09.006 - DOI
Publication types
LinkOut - more resources
Full Text Sources