

Postoperative Bleeding After the Modified Frey Procedure With Laparoscopic Distal Pancreatectomy for a Hemorrhagic Pancreatic Pseudocyst: A Case Report
- PMID: 40385787
- PMCID: PMC12085789
- DOI: 10.7759/cureus.82494
Postoperative Bleeding After the Modified Frey Procedure With Laparoscopic Distal Pancreatectomy for a Hemorrhagic Pancreatic Pseudocyst: A Case Report
Abstract
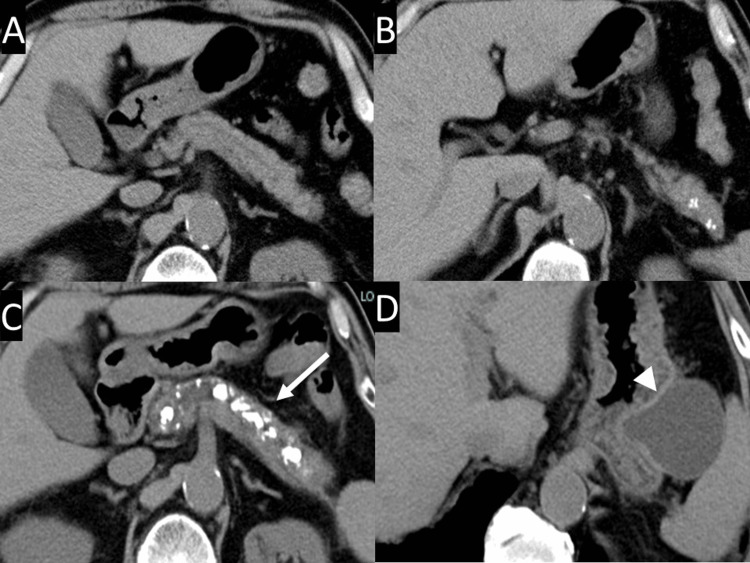
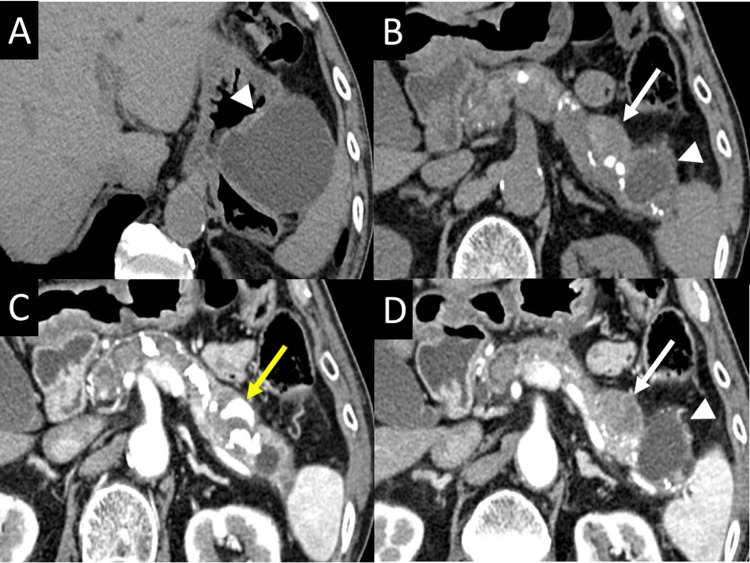
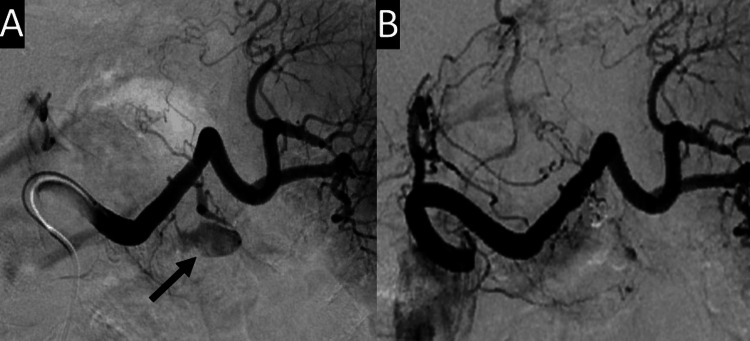
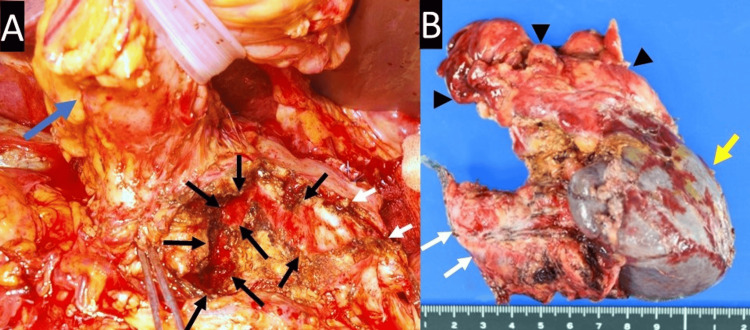
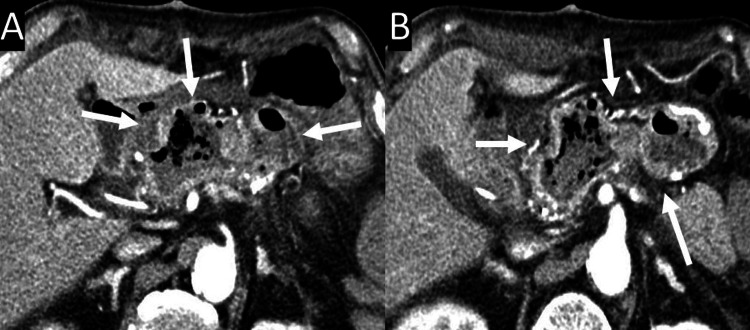
We report a case of a hemorrhagic pancreatic pseudocyst (PPC) in which a laparoscopic distal pancreatectomy and modified Frey procedure were performed. These procedures resulted in postoperative bleeding from a small hole in the pancreatic duct wall, caused by the removal of a pancreatic duct stone. A 76-year-old man had been undergoing follow-up treatment for six years for alcoholic chronic pancreatitis (CP). While the main pancreatic duct had gradually dilated, and its intraluminal stones had increased in number and size, a PPC had appeared and enlarged gradually at the distal end of the pancreatic tail. During a periodic follow-up, an abdominal computed tomography (CT) scan showed a new, small PPC at the duodenal side of the original, containing a hemorrhagic pseudoaneurysm. Abdominal angiography showed extravasation into the small PPC from arterial branches of the great pancreatic artery, which were subsequently embolized. Nine days after the arterial embolization, a modified Frey procedure with a laparoscopic distal pancreatectomy was performed. The postoperative course was uneventful until 13 days after the operation, when the patient exhibited epigastralgia and melena. An abdominal CT scan revealed hemorrhagic dilatation of the cavity of the longitudinal pancreaticojejunostomy, without pseudoaneurysms or active bleeding. Surgical exploration revealed arterial bleeding from a small hole in the pancreatic duct wall, which had been created during the removal of a pancreatic stone in a previous operation. Hemostasis was achieved through suture closure of the hole, and a pancreaticojejunostomy was performed again. The patient has been alive and well for five years since the surgery, without recurrence of pancreatitis, PPCs, or hemorrhage. The Frey procedure is one of the most common procedures for CP. During this operation, as many stones as possible are removed from the pancreatic duct, which may sometimes be incarcerated in a small branch of the pancreatic duct; therefore, a small hole is sometimes observed after their removal. However, it is unpredictable whether the hole may contact the wall of an arterial branch of the pancreas. Therefore, to prevent postoperative bleeding after the removal of pancreatic duct stones, suture closure of the hole should be considered.
Keywords: frey procedure; hemorrhagic pancreatic pseudocyst; intracystic hemorrhage; pancreatic stone; postoperative bleeding; treatment of chronic pancreatitis.
Copyright © 2025, Tsukamoto et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Successful resolution of a hemorrhagic pancreatic pseudocyst ruptured into the stomach complicating obstructive pancreatitis due to pancreatic cancer: a case report.World J Surg Oncol. 2016 Feb 24;14(1):46. doi: 10.1186/s12957-016-0812-x. World J Surg Oncol. 2016. PMID: 26911459 Free PMC article.
-
Hemorrhagic pseudocyst and pseudocyst with pseudoaneurysm successfully treated by pancreatectomy: report of three cases.J Hepatobiliary Pancreat Surg. 2000;7(4):432-7. doi: 10.1007/s005340070040. J Hepatobiliary Pancreat Surg. 2000. PMID: 11180866
-
Combination of longitudinal pancreaticojejunostomy with coring-out of the pancreatic head (Frey procedure) and distal pancreatectomy for chronic pancreatitis.Surg Today. 2019 Feb;49(2):137-142. doi: 10.1007/s00595-018-1720-1. Epub 2018 Sep 26. Surg Today. 2019. PMID: 30259156
-
Surgical therapy in chronic pancreatitis.Curr Opin Gen Surg. 1993:287-93. Curr Opin Gen Surg. 1993. PMID: 7583993 Review.
-
Early Experience with Laparoscopic Frey Procedure for Chronic Pancreatitis: a Case Series and Review of Literature.J Gastrointest Surg. 2017 May;21(5):904-909. doi: 10.1007/s11605-016-3343-4. Epub 2016 Dec 26. J Gastrointest Surg. 2017. PMID: 28025771 Review.
References
-
- A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Bradley EL 3rd. Arch Surg. 1993;128:586–590. - PubMed
-
- The natural history of pancreatic pseudocysts documented by computed tomography. Yeo CJ, Bastidas JA, Lynch-Nyhan A, Fishman EK, Zinner MJ, Cameron JL. https://pubmed.ncbi.nlm.nih.gov/2326721/ Surg Gynecol Obstet. 1990;170:411–417. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous