

Understanding the Impact of Chronic Epididymo-Orchitis and Chronic Prostatitis on Testicular Volume, Testosterone Levels, Semen Quality, and Sexual Function: A Prospective, Descriptive Study
- PMID: 40385846
- PMCID: PMC12085772
- DOI: 10.7759/cureus.82482
Understanding the Impact of Chronic Epididymo-Orchitis and Chronic Prostatitis on Testicular Volume, Testosterone Levels, Semen Quality, and Sexual Function: A Prospective, Descriptive Study
Abstract
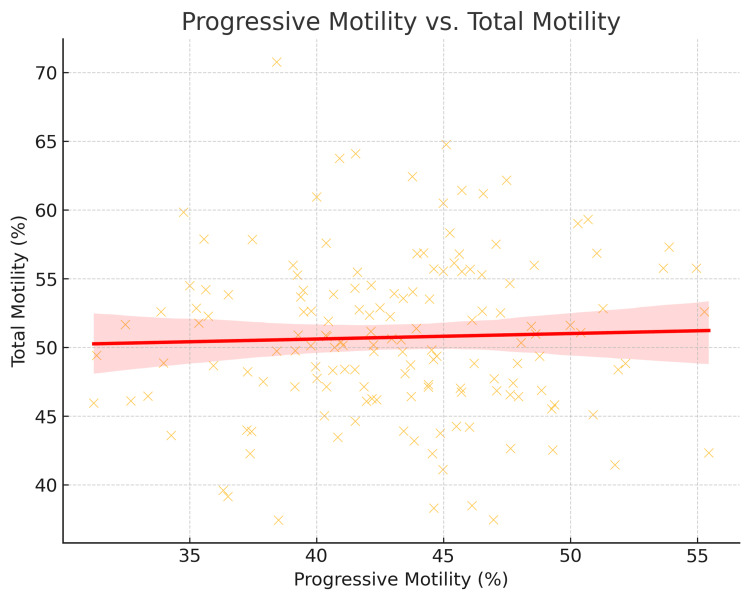
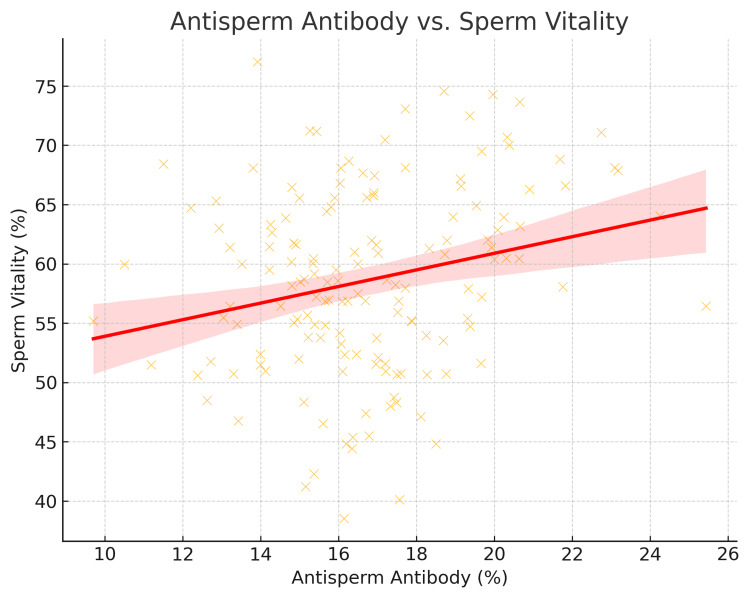
Introduction Chronic epididymo-orchitis (CEO) and chronic prostatitis (CP) are prevalent urological conditions that significantly impact male reproductive health. Despite their high prevalence, comprehensive studies evaluating their combined effects on testicular volume, testosterone levels, semen quality, and sexual function are limited. This study aims to bridge this gap by adopting an integrated approach to assess how these conditions influence these key parameters and their interrelationships. Methods This study was conducted at the Department of Urology, Institute of Post Graduate Medical Education & Research (IPGEMR), Kolkata, India, from February 2024 to January 2025. Male patients aged 18-60 years diagnosed with CEO and/or CP were recruited. Participants underwent baseline evaluations, including medical history, physical examination, blood tests for testosterone levels, semen analysis, and ultrasound imaging to assess testicular volume. Sexual function was assessed using a structured questionnaire developed based on established domains of male sexual function, including erectile function, sexual desire, orgasmic function, intercourse satisfaction, and overall satisfaction. Data were analyzed using descriptive and comparative statistical methods. Results The study included 153 participants, with 48 diagnosed with CEO and 105 with CP. The preliminary findings revealed several important insights. There was a significant reduction in both testicular volume and testosterone levels in men with CEO and CP, suggesting an association between these conditions and testicular atrophy and hormonal imbalances. Semen analysis showed a decrease in sperm count, motility, and morphology, indicating that CEO and CP can negatively affect fertility by impairing sperm quality. The structured questionnaire used to assess sexual function revealed that many participants experienced erectile dysfunction and painful ejaculation, which are common symptoms of these conditions. The study also found that changes in one parameter, such as testosterone levels, could influence others, like sexual function or semen quality. For example, lower testosterone levels were associated with poorer sexual function and reduced sperm quality. Conclusion This study is unique in its comprehensive approach to evaluating the multifaceted impact of CEO and CP on male reproductive health. By this integrated approach, this study contributes to a deeper understanding of the clinical manifestations and long-term consequences of these chronic urological conditions, particularly how each parameter (testicular volume, testosterone levels, semen quality, and sexual function) affects the others. The findings highlight the need for further research to explore the complex interrelationships between these parameters and their implications for male reproductive health.
Keywords: chronic epididymo-orchitis; chronic urological conditions; hormonal imbalance and male infertility; male reproductive health; questionnaire used to assess sexual function; sperm morphology; sperm motility; testicular volume testosterone levels semen quality sexual function erectile dysfunction testicular atrophy; ultrasound imaging testicular volume; urology andrology sexual health testosterone chronic prostatitis.
Copyright © 2025, Mondal et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Ethics Committee of Institute of Post Graduate Medical Education & Research, Kolkata issued approval IPGME&R/IEC/2024/0232. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures





References
-
- Research guidelines for chronic prostatitis: consensus report from the first National Institutes of Health International Prostatitis Collaborative Network. Nickel JC, Nyberg LM, Hennenfent M. Urology. 1999;54:229–233. - PubMed
-
- The NIH Consensus concept of chronic prostatitis/chronic pelvic pain syndrome compared with traditional concepts of nonbacterial prostatitis and prostatodynia. Krieger JN, Ross SO, Deutsch L, Riley DE. Curr Urol Rep. 2002;3:301–306. - PubMed
-
- Overview summary statement. Diagnosis and management of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) Schaeffer AJ, Landis JR, Knauss JS. J Urol. 2002;168:593–598. - PubMed
-
- Implications of prostate inflammation on male fertility. Motrich RD, Salazar FC, Breser ML, et al. Andrologia. 2018;50:0. - PubMed
-
- Treatment of acute epididymitis: a systematic review and discussion of the implications for treatment based on etiology. Louette A, Krahn J, Caine V, Ha S, Lau TT, Singh AE. Sex Transm Dis. 2018;45:0–8. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous