

Total Knee Arthroplasty for Severe Crystalline-Induced Arthropathy: A Case Report From a Third-Level Hospital
- PMID: 40385933
- PMCID: PMC12085199
- DOI: 10.7759/cureus.82462
Total Knee Arthroplasty for Severe Crystalline-Induced Arthropathy: A Case Report From a Third-Level Hospital
Abstract
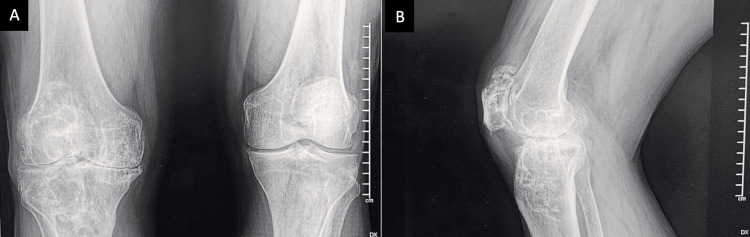
Gout is an inflammatory arthritis caused by monosodium urate crystal deposition, leading to progressive joint destruction and functional impairment. While pharmacologic treatment remains the standard, advanced cases with intra-articular and intraosseous tophi may require surgical intervention. Total knee arthroplasty (TKA) has been reported as a viable option for managing severe tophaceous gout with structural bone defects, improving joint function and pain control when conservative therapy fails. We present the case of a 56-year-old male with a long-standing history of gout and progressive knee pain refractory to medical treatment. Imaging revealed extensive intraosseous tophi with cavitary bone defects, prompting the decision for TKA with bone allograft reconstruction. The patient experienced favorable postoperative recovery, demonstrating significant improvement in joint mobility and function, with no complications observed. This case highlights the role of surgical intervention in the management of advanced tophaceous gout as part of an integrated approach alongside pharmacologic control.
Keywords: arthroplasty; gout disease; joint replacement surgeon; knee arthroplasty; knee replaecment.
Copyright © 2025, Hernández-Penagos et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Hospital Regional Elvia Carrillo Puerto, Institute for Social Security and Services for State Workers (ISSSTE) issued approval RPI/HRECP/078. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures





References
Publication types
LinkOut - more resources
Full Text Sources