

Safety and clinical efficacy of Relmacabtagene autoleucel (relma-cel) for systemic lupus erythematosus: a phase 1 open-label clinical trial
- PMID: 40386685
- PMCID: PMC12083988
- DOI: 10.1016/j.eclinm.2025.103229
Safety and clinical efficacy of Relmacabtagene autoleucel (relma-cel) for systemic lupus erythematosus: a phase 1 open-label clinical trial
Abstract
Background: Systemic lupus erythematosus (SLE) is a classic systemic autoimmune disease mediated by autoantibodies. Chimeric antigen receptor T (CAR-T) cell therapy, known for its success in cancer, has shown promise in achieving durable B cell depletion and long-term remission in SLE. Relmacabtagene autoleucel (relma-cel) is the second anti-CD19 CAR-T product approved for marketing by the National Medical Products Administration (NMPA) in China and demonstrates its long-term efficacy in relapsed/refractory (r/r) large B cell lymphoma (LBCL). We report the results from a phase I open-label clinical trial of relma-cel in treating patients with moderately to severely active SLE.
Methods: Eligible patients were aged 18-70 years, a ≥6-month history of SLE, and the disease had to remain active after at least 2 months of stable SLE standard treatment prior to screening. We evaluated four dose levels (DL) of relma-cel in a dose-escalation scheme: total dose of 25 × 106, 50 × 106, 75 × 106, and 100 × 106 anti-CD19 CAR-T cells. All patients received lymphodepletion chemotherapy with fludarabine and cyclophosphamide. The primary endpoints were the incidence of dose-limiting toxicities (DLTs) and adverse events (AEs). Secondary endpoints included the evaluation of standard cellular pharmacokinetic parameters, the SLE Responder Index (SRI) response rate, and changes from baseline in the Safety of Estrogens in Lupus Erythematosus National Assessment-Systemic Lupus Erythematosus Disease Activity Index (SELENA-SLEDAI), British Isles Lupus Assessment Group 2004 (BILAG-2004) and Physician's Global Assessment (PGA) scores post-treatment. This trial is registered with ClinicalTrials.gov, NCT05765006.
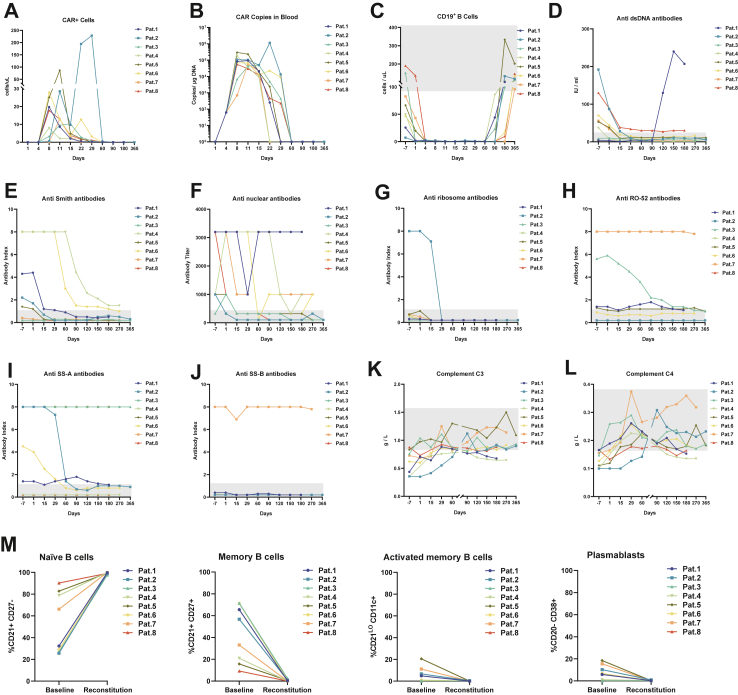
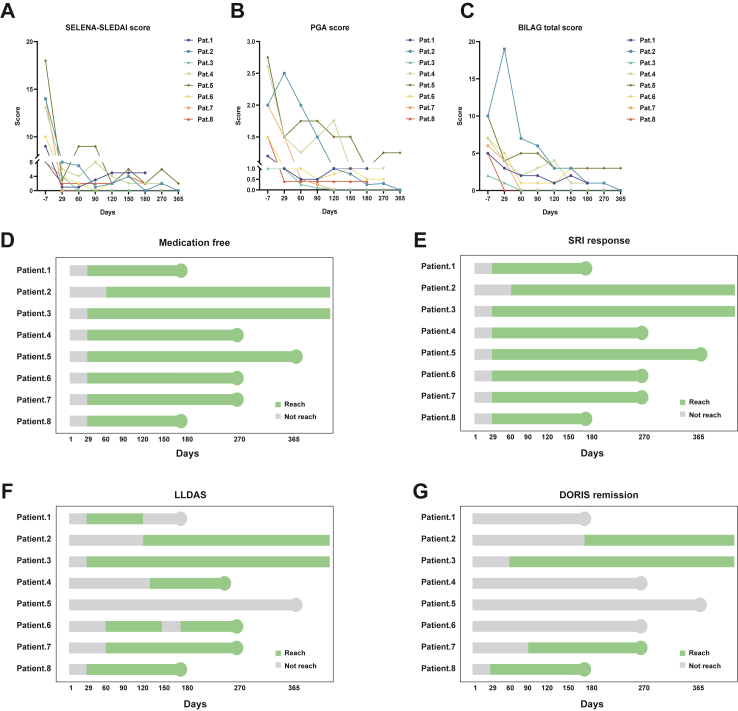
Findings: Between March 28, 2023 and April 8, 2024, a total of 12 patients were screened for study inclusion, of whom 8 patients were enrolled and assigned to different dose levels: 25 × 106 cells (n = 3), 50 × 106 cells (n = 2), 75 × 106 cells (n = 2), and 100 × 106 cells (n = 1). No DLT was observed. The most common AEs included cytopenia (n = 8, 100%), cytokine release syndrome (CRS) (n = 7, 88%) and hypogammaglobulinemia (n = 5, 63%). No Grade 3 or higher immune effector cell-associated hematotoxicity (ICAHT) occurred. No cases of immune effector cell-associated neurotoxicity syndrome (ICANS) were reported. CRS was predominantly grade 1, characterized mainly by mild fever and muscle soreness. A rare severe adverse event, immune effector cell-associated hemophagocytic lymphohistiocytosis-like syndrome (IEC-HS), was observed in one patient. The median time to reach maximum CAR-T cell expansion (Cmax) was 9.5 days (range: 8-22 days). The median Cmax was 18.74 CD3+CAR+ cells/μL (range: 7.94-228.36) by flow cytometry and 81766.5 copies/μg DNA (range: 50,979-1,140,893) by quantitative real-time PCR (qPCR). In all patients treated with relma-cel, CD19+ B cells in peripheral blood were almost completely depleted within 11-15 days and gradually recovered within 2-6 months. All patients achieved SRI response. Four patients achieved Definition of Remission in SLE (DORIS) remission criteria and seven patients reached the Lupus Low Disease Activity State (LLDAS) criteria within 1-4 months following relma-cel infusion.
Interpretation: This study preliminarily demonstrated that relma-cel is an effective and safe CAR-T product for the treatment of patients with moderately to severely active SLE, providing valuable clinical insights into the management of rare complications. Further studies with larger sample sizes are warranted.
Funding: National Natural Science Foundation of China.
Keywords: Anti-CD19 CAR-T cell; Clinical efficacy; Safety; Systemic lupus erythematosus.
© 2025 The Author(s).
Conflict of interest statement
All co-authors declare no competing interests. JW Therapeutics (Shanghai) Co., Ltd. provided the investigate drugs (relma-cel) and financial support throughout the clinical trial, such as patient compensation and the examination costs. The other work in this clinical trial, including study design, data collection, data analysis, data interpretation and writing of the report et al. were jointly conducted by authors. The company has no objection to the contributions described in the manuscript, and there are no conflicts of interest between the company and all co-authors.
Figures


References
-
- Kamburova E.G., Koenen H.J.P.M., Borgman K.J.E., ten Berge I.J., Joosten I., Hilbrands L.B. A single dose of rituximab does not deplete B cells in secondary lymphoid organs but alters phenotype and function. Am J Transplant. 2013;13(6):1503–1511. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
