

Predictors of iatrogenic atrial septal defects: analysis of fibrotic atrial cardiomyopathy, valvular disease, and transseptal sheath size
- PMID: 40388037
- PMCID: PMC12317873
- DOI: 10.1007/s10840-025-02065-0
Predictors of iatrogenic atrial septal defects: analysis of fibrotic atrial cardiomyopathy, valvular disease, and transseptal sheath size
Abstract
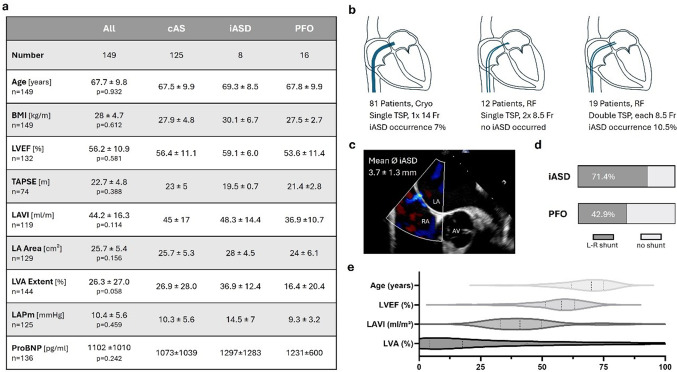
Background: Transseptal puncture (TSP) for left atrial access is routinely used during various cardiac interventions, including ablation for atrial tachyarrhythmia. However, in selected patients, subsequent iatrogenic atrial septal defects (iASD) persist. This study determines whether fibrotic atrial cardiomyopathy (FACM) or mitral valve regurgitation (MR) are predictors of persistent iASD development post-TSP.
Methods: We analyzed data from patients undergoing radiofrequency ablation with high-density electroanatomical mapping for recurrent atrial tachyarrhythmias after a primary pulmonary vein isolation using either cryo or RF technologies. Patients were categorized based on transesophageal echocardiography findings: (1) competent atrial septum (cAS) (2), iASD, or (3) a patent foramen ovale (PFO). Differences in FACM and MR were assessed across these groups.
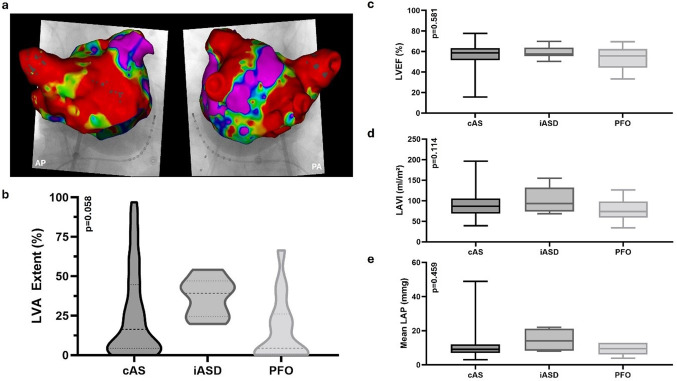
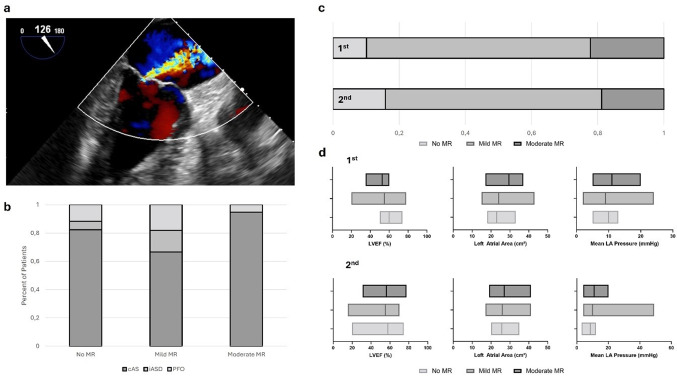
Results: Of 149 patients (age 67.7 ± 9.7 years), 125 (83.9%) had cAS, 8 (5.4%) iASD, and 16 (10.7%) PFO. No significant differences were observed in age (p = 0.932), BMI (p = 0.612), or LVEF (p = 0.581). The TSP sheath size was not associated with iASD occurrence (p = 0.857). Common surrogates of FACM, i.e., LAVI (p = 0.114), LA area (p = 0.156), mean left atrial pressure (LAP; p = 0.459), or total low-voltage area burden (p = 0.058) did not differ significantly among groups. MR was not linked to increased LAP (at first (p = 0.290) and second procedure (p = 0.212)) or a higher incidence of iASD (at first (p = 0.155) and second procedure (p = 0.917)). Mean LAP did not correlate with LA size (p = 0.471) or low-voltage extent (p = 0.084).
Conclusion: Our findings underscore that iASDs post-TSP for left atrial ablation are uncommon and unrelated to TSP sheath size, FACM, or MR, further minimizing concerns for routine interventions in patients with more advanced arrhythmia substrate or valvular disease.
Keywords: Ablation; Atrial cardiomyopathy; Atrial fibrillation; Atrial septal defect; Transseptal puncture.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare they have no financial interests regarding the submitted work. EH received travel grants outside the submitted work from Bayer, Edwards LifeSciences, Medtronic, and Pfizer.
Figures
Similar articles
-
Transseptal puncture for catheter ablation of atrial fibrillation in patients with septal occluder devices.Heart Rhythm. 2025 Sep;22(9):e578-e585. doi: 10.1016/j.hrthm.2025.03.1996. Epub 2025 Apr 3. Heart Rhythm. 2025. PMID: 40187509
-
Analysis of healing status and influencing factors of iatrogenic atrial septal defect in patients with atrial fibrillation after cryoballoon ablation.Eur J Med Res. 2025 Jul 10;30(1):612. doi: 10.1186/s40001-025-02875-y. Eur J Med Res. 2025. PMID: 40640982 Free PMC article.
-
Incidence and predictors of persistent iatrogenic atrial septal defect following catheter ablation.J Cardiol. 2024 Dec;84(6):372-378. doi: 10.1016/j.jjcc.2024.06.007. Epub 2024 Jun 22. J Cardiol. 2024. PMID: 38914280
-
Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evaluation.Health Technol Assess. 2008 Nov;12(34):iii-iv, xi-xiii, 1-198. doi: 10.3310/hta12340. Health Technol Assess. 2008. PMID: 19036232
-
Iatrogenic atrial septal defect following transseptal cardiac interventions.Int J Cardiol. 2016 Apr 15;209:142-8. doi: 10.1016/j.ijcard.2016.02.068. Epub 2016 Feb 6. Int J Cardiol. 2016. PMID: 26894464 Review.
References
-
- Ross J Jr., Braunwald E, Morrow AG. Transseptal left atrial puncture; new technique for the measurement of left atrial pressure in man. Am J Cardiol. 1959;3(5):653–5. - PubMed
-
- Brockenbrough EG, Braunwald E. A new technic for left ventricular angiocardiography and transseptal left heart catheterization. Am J Cardiol. 1960;6(6):1062–4.
-
- Alkhouli M, Rihal CS, Holmes DR. Transseptal techniques for emerging structural heart interventions. JACC: Cardiovasc Interventions. 2016;9(24):2465–80. - PubMed
-
- Singh SM, Douglas PS, Reddy VY. The Incidence and Long-Term Clinical Outcome of Iatrogenic Atrial Septal Defects Secondary to Transseptal Catheterization With a 12F Transseptal Sheath. Circulation: Arrhythmia and Electrophysiology. 2011;4(2):166– 71. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
