

Glycaemic and Weight Control in People Aged 65 or Younger Newly Diagnosed with Type 2 Diabetes in Spain: Insights from the PRIORITY-T2D Study
- PMID: 40388088
- PMCID: PMC12182470
- DOI: 10.1007/s12325-025-03230-7
Glycaemic and Weight Control in People Aged 65 or Younger Newly Diagnosed with Type 2 Diabetes in Spain: Insights from the PRIORITY-T2D Study
Abstract
Introduction: The objective of this study was to determine the number of people within glycated haemoglobin (HbA1c) targets and achieving weight-loss goals during the first 5 years after type 2 diabetes (T2D) diagnosis and to explore the relationship between early weight loss and glycaemic control in routine care in Spain.
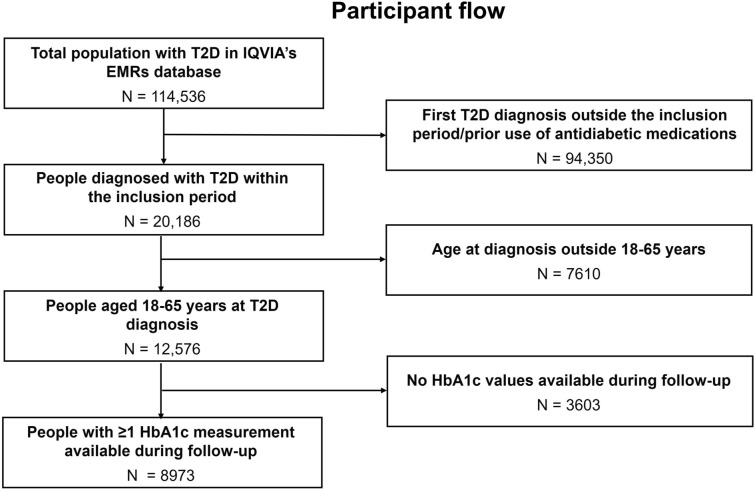
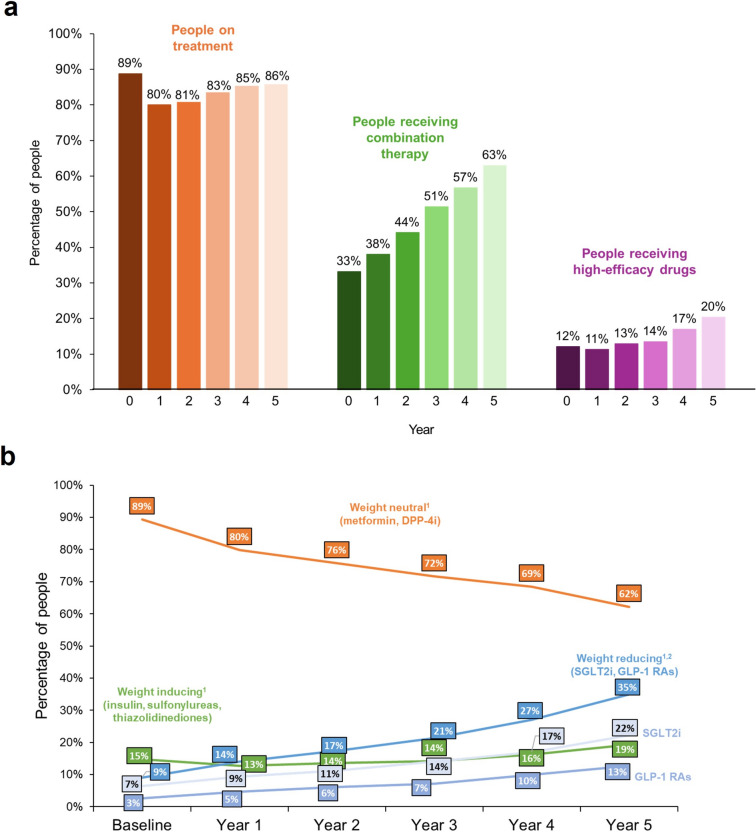
Methods: This was an observational retrospective study using IQVIA's electronic medical record database, including adults aged ≤ 65 years newly diagnosed with T2D. Variables included baseline sociodemographic/clinical characteristics, yearly HbA1c and weight data, and treatment patterns. Descriptive statistics and regression analyses were used.
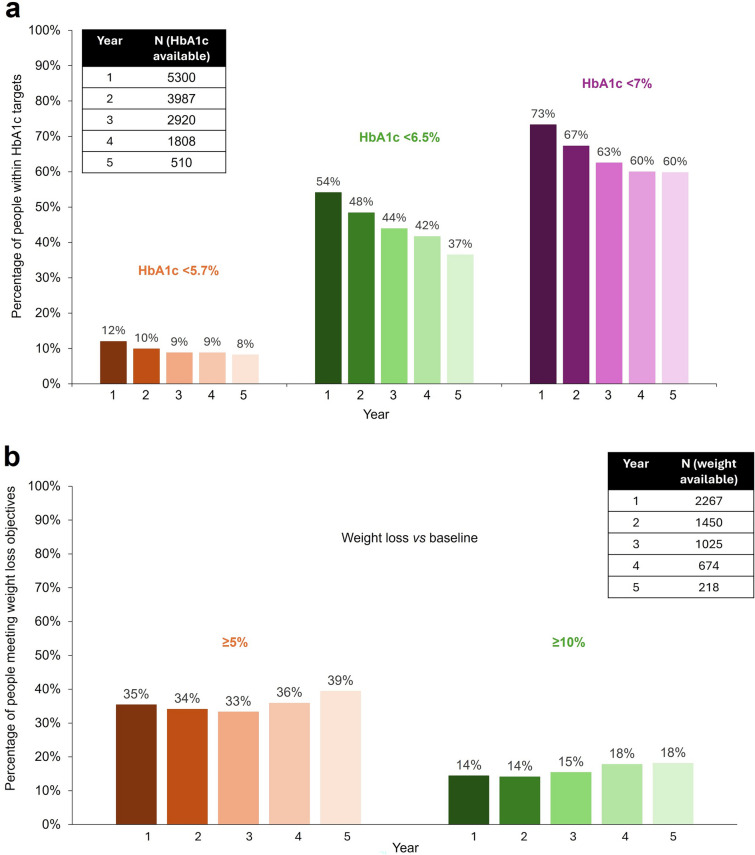
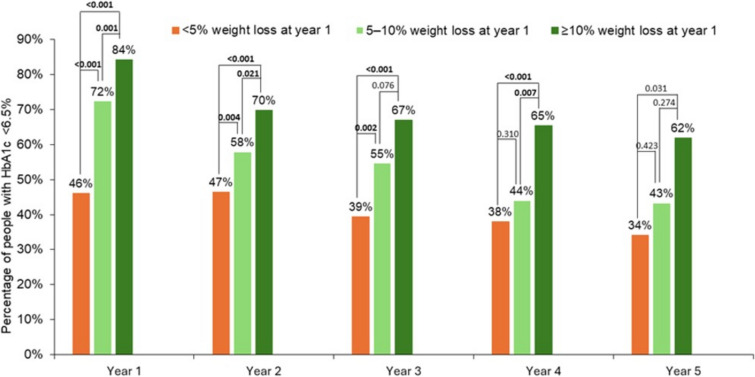
Results: A total of 8973 people with T2D were included (mean age 53 years; mean baseline HbA1c 7.7%; obesity at diagnosis: 64%). During the first 5 years post-T2D diagnosis, 46-63% of the population did not have HbA1c < 6.5%, and > 60%, and > 80% of subjects did not achieve ≥ 5% and ≥ 10% weight loss, respectively. Early weight loss goal achievement (1st year after diagnosis) and weight loss magnitude were associated with a higher percentage of people with HbA1c < 6.5%.
Conclusions: Many individuals with T2D did not have HbA1c < 6.5% in the first 5 years after diagnosis and did not achieve ≥ 5% or ≥ 10% weight loss. Early weight loss after T2D diagnosis was associated with higher likelihood of achieving early glycaemic control.
Keywords: Glycated haemoglobin; Health outcomes; Spain; Treatment patterns; Type 2 diabetes; Weight loss.
Plain language summary
This study looked at how many people with type 2 diabetes met blood glucose targets and weight-loss goals in the first 5 years after their diagnosis. It also explored the link between early weight loss and blood glucose control in regular healthcare settings in Spain. Researchers analysed data from electronic medical records, focussing on adults aged 65 or younger who were newly diagnosed with diabetes. The study looked at the characteristics of people with diabetes, yearly blood glucose levels (as reflected in their glycated haemoglobin levels), weight measurements, and treatment patterns. The study used statistical methods to summarise the data and find connections. The study included 8973 people with newly diagnosed type 2 diabetes, with an average age of 53 years and an average starting glycated haemoglobin of 7.7%. About 64% had obesity at diagnosis. Over the first 5 years, 46–63% of people did not achieve glycated haemoglobin levels below 6.5%. Guidelines recommend glycated haemoglobin levels equal or below 7.0%, or 6.5% for people who can achieve this goal safely. Additionally, more than 60% did not lose at least 5% of their weight, and more than 80% did not lose at least 10%. Those who lost weight within the first year after diagnosis and lost more weight overall were more likely to achieve good blood glucose control. This study concluded that many people with type 2 diabetes did not achieve their blood glucose or weight-loss goals within 5 years of diagnosis. However, losing a meaningful amount of weight early on was linked to better blood glucose control early in the disease.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflicts of Interest: Emilio Ortega has received institutional grants from Eli Lilly and Novo Nordisk, consulting fees from Eli Lilly, honoraria for presentations, manuscript writing or educational events from Eli Lilly and Novo Nordisk, and support for meeting attendance and/or travel from Eli Lilly and Novo Nordisk. Jennifer Redondo-Antón, Silvia Díaz-Cerezo, Miriam Rubio-de Santos, and Irene Romera are employees and minor shareholders of Eli Lilly and Company, Spain. Ethical Approval: As this was an observational study that used previously collected data and did not impose any form of intervention, and the data were previously deidentified/anonymised to protect participant privacy, a formal Consent to Release Information form was not required. Permission was obtained to access and use data from this database. The study protocol was approved by the ethical review board of Hospital Clinic (Barcelona, Spain) (approval code HCB/2023/0287, dated 16 May 2023), as required by Spanish regulations related to healthcare observational studies. The study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki and are consistent with Good Pharmacoepidemiology Practices and applicable laws and regulations of Spain.
Figures
Similar articles
-
Treatment of periodontitis for glycaemic control in people with diabetes mellitus.Cochrane Database Syst Rev. 2022 Apr 14;4(4):CD004714. doi: 10.1002/14651858.CD004714.pub4. Cochrane Database Syst Rev. 2022. PMID: 35420698 Free PMC article.
-
Newer agents for blood glucose control in type 2 diabetes: systematic review and economic evaluation.Health Technol Assess. 2010 Jul;14(36):1-248. doi: 10.3310/hta14360. Health Technol Assess. 2010. PMID: 20646668
-
Quality improvement strategies for diabetes care: Effects on outcomes for adults living with diabetes.Cochrane Database Syst Rev. 2023 May 31;5(5):CD014513. doi: 10.1002/14651858.CD014513. Cochrane Database Syst Rev. 2023. PMID: 37254718 Free PMC article.
-
Continuous glucose monitoring systems for type 1 diabetes mellitus.Cochrane Database Syst Rev. 2012 Jan 18;1(1):CD008101. doi: 10.1002/14651858.CD008101.pub2. Cochrane Database Syst Rev. 2012. PMID: 22258980 Free PMC article.
-
Effect of weight reduction on glycated haemoglobin in weight loss trials in patients with type 2 diabetes.Diabetes Obes Metab. 2017 Sep;19(9):1295-1305. doi: 10.1111/dom.12971. Epub 2017 May 22. Diabetes Obes Metab. 2017. PMID: 28417575
References
-
- Samson SL, Vellanki P, Blonde L, et al. American Association of Clinical Endocrinology consensus statement: comprehensive type 2 diabetes management algorithm - 2023 Update. Endocr Pract. 2023;29:305–40. 10.1016/j.eprac.2023.02.001. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
